COVID-19 fought by Vitamin D in 43 studies
Vitamin D Mitigates COVID-19, Say 40+ Patient Studies (listed below) – Yet BAME, Elderly, Care-homers, and Obese are still ‘D’ deficient, thus at greater COVID-19 risk - WHY?
British Medical Journal Oct 15, 2020
Robert A Brown, Researcher, McCarrison Society, La Route de Mont Cochon, St Lawrence, Jersey. C.I. @purplejustice
Dear Editor
Vitamin D reduces COVID-19; infection; severity; ICU admission and mortality: as clearly evidenced by; immune biology, observational and interventional studies, and wider considerations of; latitude, seasonal UVB exposure, and national supplementation policies: the uncertainty is the quantum: but studies suggest ‘D’ effects are likely large - 50% less infectivity – multiples lower ICU and mortality rate.
Vitamin D is a steroid hormone, also present in limited dietary sources. For most, the major ‘D’ source is skin exposure to UVB in sunlight, which waxes and wanes seasonally. Supplementation is the only other option. ‘D’ with 50 metabolites[1] is more bio-actively influential than appreciated. Sensible ‘D’ supplementation has a 100-year track-record.[2] Side-effects are minimal.
Dexamethasone in the same structural steroid family as ‘D’, shares common VDR (vitamin-D-receptor)[3] and related gene pathways,[4] is artificial, and in some circumstances mitigates against COVID-19, albeit with variable side-effects. Dexamethasone is clearly a useful adjunct.
‘D’ deficiencies are widespread globally,[5] and particularly in; BAME, African Americans, Elderly, Carehomers,[6, 7] (Reality-check ref.) and Obese Persons; groups also at high-risk of COVID-19. Regions with proactive Vitamin-D-policies, education, nutritional supplementation, and/or greater UVB exposure, have much lower COVID-19 infection and mortality; e.g. Finland, Norway, New Zealand and, Equatorial-Africa (despite poverty / high urban-multi-person-dwelling-occupation).
Appropriate vitamin D supplementation risks are small: rewards huge. Public policy application of Bradford-Hill risk / harm criteria, used for smoking, social-distancing and masks, would support[8] ‘D’ supplementation of at-risk groups, and ‘D’ testing of all COVID-19 hospital patients.
Parachute RCTs studies (Smith & Pell. J CBE[9] ) [10, 11] ; analogies for research situations of observable risk reduction, but limited viable ethical alternatives; incisively, with wry humour, highlight risks of overly focusing on para-RCT-centric research.
Patient-based-studies
four interventions [12-14, 85];
a retrospective examination of clinical practice[15]; and
thirty-nine observationals, [16-50, 86]
three more are questioned;[51-53]
- some are preprints.
All consider, mixed-size pre-and -or-post-infection ‘D’ samples, and COVID-19 positive patients. All studies variously evidence mitigation of COVID-19 infectivity and/or severity, by ‘D’.
Additionally, Biobank-study ‘D’ data (all over 10-years-old),[54-56] showed positive associations before adjustment. Comorbidities adjusted for, are impacted by vitamin D levels,[57] making evaluation complex. EPIC vitamin D data had no date-limits.[58]
Latitudinal,[59] COVID-19 seasonality, and wider, studies, including of polymorphisms,[60] grow in number; including those referencing historic pandemics and influenzas[61]: Juzeniene is a stand-out.[62] Latitudinal studies[63, 64] are helpful, but limited by availability of current accurate population ‘D’ data.
An in-vitro study,[65] observes; “Vitamin D, calcitriol, exhibits significant potent activity against SARS-CoV-2.”
Numerous studies,[66] explain vitamin D’s central genetic evolutionary,[67, 68] and wider role, in immune modulation, through multiple various and diverse [69] pathways, including via peroxisomes and mitochondria. More generally, studies link low ‘D’ with negative wider health effects[70] including increased mortality.[71]
Early 2020 hypotheses linking COVID-19 infectivity / severity, to vitamin D, include; Grant,[72] Brown,[73] and Davies.[74] Helpful summaries include Benskin.[75]
The urgent need for major studies, has been raised in several BMJ Rapid Responses.[76-82]
Collectively, studies strongly suggest essential prohormone-and-nutrient vitamin D, is a far more effective potential basal COVID-19 treatment, than any additive pharmaceutical available to date. Pharmaceuticals and vaccines are ultimately appreciated adjuncts, to meeting essential evolutionary biological nutrient intake imperatives.
Immediately testing of all COVID-19 hospital patient admissions for vitamin D, and supplementing where necessary, according to established NICE guidelines,[83] would provide time for new protocol, RCT-clinical-trials.
Thus, there is every reason to ‘D’ test hospitalised COVID-19 patients. Arguably, not to do so, in light of study outcomes to date, risks negligence. Judges, if asked, may take a broad-view in weighing evidence.
Since late January 2020, a loose group, have requested major clinical studies of sufficient power, including in care-homes, and hospitals. I thank Cooper, Grant, Grimes, Lahore, Pfleger, Rhein, Shotwell, Sarkar, and others, for sharing.
However, high-level drive and funding, have been lacking, exacerbated by the Wellcome-Gates-Accelerator exclusion from funding of ‘D’. Consequentially, research establishments excluded ‘D’ trials, focusing instead on repurposing, and new drugs, including in care-home settings. ‘D’ studies would reduce the study patient pool: further, successful ‘D’ outcomes may reduce funding for long-shot studies.
‘D’ is a non-patentable product family, produced by evolution, for which humans can garner no credit, with limited financial drivers to satisfy eternal human-yearning for golden but elusive bonanzas.
Overall, if the depth of information, and number of studies on ‘D’, consistently pointing in the same direction, related to a new COVID-19 ‘drug’, with minimal side-effects, it would have been front-page-news. Additional clinical research would have been prioritised with determination and alacrity, and ‘D’ by now, licensed as a standard-treatment-protocol.
In terms of saving lives, mental health and economies, it is inconsequential whether deficiency is due to pre-existing low-levels at infection, or infection driven catabolism. IF the issue was dehydration, nobody would dream of saying, ‘withhold treatment until determination if dehydration was due to; fever, or low historic water intake pre-infection’.
Surely the simple steps, of ‘D’ supplementing, and/or testing-and-supplementing, of at least all COVID-19 patients, and high-risk-persons, should be implemented as a matter of urgency. Thought-provokingly hospital ‘D’ supplementation was standard practice in Daniel Drake Center for Post-Acute Care in Cincinnati for many years.[84]
Absent: authorities; redirecting resources and research-focus; changing public health and hospital testing and supplementation policies, to ones that fully recognise the often-discriminatory impact and extent of ‘D’ deficiency disease, particularly in high risk groups; and funding and driving of urgent further ‘D’ research; human-frailties dictate ‘D’ will be shuffled into the pending-tray; notwithstanding observed 50% ‘D’ related reductions in infection (Kaufman 190,000 patient-base),[27, 39, 41] and reductions in ICU patients by multiples (Castillo, Tan et al).[12, 17, 31, 45, 48]
Pragmatic recognition of the need to: supplement ‘D’ in; high risk groups, COVID-19 hospital patients, and more widely; eliminate the ‘social-injustice’[6, 7] of vitamin ‘D’ discrimination against; BAME, the Elderly, Carehomers and Obese; reduce infection, ICU pressures and mortality, so public fear: could provide a cheap resource-and-cost-saving basal treatment protocol, added to by vaccines, a ‘paradigm-shift’ enlightening bleak COVID-19 outlooks, empowering people, thus possible exit from D-deficient COVID-19 pandemic shadow-lands, steering a ‘D’ course to a brighter pastures.
References
1] Kattner. L., & Volmer D. (11th Nov 2015) Synthesis of Low Abundant Vitamin D Metabolites and Assaying Their Distribution in Human Serum by Liquid Chromatography-Tandem Mass Spectrometry (LCMS/MS) as a New Tool for Diagnosis and Risk Prediction of Vitamin D-Related Diseases http://dx.doi.org/10.5772/64518 Available at https://www.intechopen.com/books/a-critical-evaluation-of-vitamin-d-basi...
2] Wolf, G. (June 2004) The Discovery of Vitamin D: The Contribution of Adolf Windaus, The Journal of Nutrition, Volume 134, Issue 6, Pages 1299–1302, https://doi.org/10.1093/jn/134.6.1299 Available at https://academic.oup.com/jn/article/134/6/1299/4688802
3] Hidalgo, A., Trump, D., & Johnson, C. (2010). Glucocorticoid regulation of the vitamin D receptor. The Journal of steroid biochemistry and molecular biology, 121(1-2), 372–375. https://doi.org/10.1016/j.jsbmb.2010.03.081 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907065/
4] Navarro-Barriuso, J., Mansilla, M.J., Naranjo-Gómez, M. et al. (2018). (Fig. 3) Comparative transcriptomic profile of tolerogenic dendritic cells differentiated with vitamin D3, dexamethasone and rapamycin. Sci Rep 8, 14985 (2018). https://doi.org/10.1038/s41598-018-33248-7 Available at https://www.nature.com/articles/s41598-018-33248-7
5] Palacios, C., & Gonzalez, L. (2014). Is vitamin D deficiency a major global public health problem? The Journal of steroid biochemistry and molecular biology, 144 Pt A, 138–145. https://doi.org/10.1016/j.jsbmb.2013.11.003 Available at https://www.intechopen.com/books/a-critical-evaluation-of-vitamin-d-basi...
6] Lay, C. (13th October 2020 ). Care homes ‘should give Vitamin D to residents’. The Times. Available at https://www.thetimes.co.uk/article/care-homes-should-give-vitamin-d-to-r...
7] Williams J, Williams C. ( 2020 ). Responsibility for vitamin D supplementation of elderly care home residents in England: falling through the gap between medicine and food. BMJ Nutrition, Prevention & Health 2020;bmjnph-2020-000129. doi: 10.1136/bmjnph-2020-000129 Available at https://nutrition.bmj.com/content/early/2020/09/20/bmjnph-2020-000129
8] Annweiler, C., Zhijian, C., & Sabatier, J. (June 07, 2020 ). Point of view: Should COVID-19 patients be supplemented with vitamin D? Maturitas. Review article, Volume 140, P24-26, DOI:https://doi.org/10.1016/j.maturitas.2020.06.003 Available at https://www.maturitas.org/article/S0378-5122(20)30292-9/fulltext
9] Pell, J. NIH List of publications. Available at https://pubmed.ncbi.nlm.nih.gov/?term=Pell%20JP%5BAuthor%5D&cauthor;=true...
10] Smith, G., & Pell, J. (2003). Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ (Clinical research ed.), 327(7429), 1459–1461. https://doi.org/10.1136/bmj.327.7429.1459 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC300808/
11] Yeh R, Valsdottir L, Yeh M, Shen C, Kramer D, et al. PARACHUTE Investigators. (13th December 2018) Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial. BMJ. 2018 Dec 13;363:k5094. doi: 10.1136/bmj.k5094. Erratum in: BMJ. 2018 Dec 18;363:k5343. PMID: 30545967; PMCID: PMC6298200. Available at https://pubmed.ncbi.nlm.nih.gov/30545967/
12] Entrenas Castillo, M., Entrenas Costa, L., Vaquero Barrios, J., Alcalá Díaz, J., López Miranda, J., Bouillon, R., & Quesada Gomez, J. (29th August 2020 ). Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. The Journal of steroid biochemistry and molecular biology, 203, 105751. https://doi.org/10.1016/j.jsbmb.2020.105751 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7456194/
13] Ohaegbulam, K., Swalih, M., Patel, P., Smith, M., & Perrin, R. (13th Aug 2020 ). Vitamin D Supplementation in COVID-19 Patients: A Clinical Case Series. American journal of therapeutics, 27(5), e485–e490. https://doi.org/10.1097/MJT.0000000000001222 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7473790/
14] Tan, C., Ho, L., Kalimuddin, S., Cherng, B., Teh, Y., et.al. (10th June 2020 ) A cohort study to evaluate the effect of combination Vitamin D, Magnesium and Vitamin B12 (DMB) on progression to severe outcome in older COVID-19 patients. doi: https://doi.org/10.1101/2020.06.01.20112334 Available at https://www.medrxiv.org/content/10.1101/2020.06.01.20112334v2
15] Panagiotou, G., Tee, S. A., Ihsan, Y., Athar, W., Marchitelli, G., Kelly, D., Boot, C. S., Stock, N., Macfarlane, J., Martineau, A. R., Burns, G., & Quinton, R. ( 2020 ). Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalized with COVID-19 are associated with greater disease severity. Clinical endocrinology, 10.1111/cen.14276. Advance online publication. https://doi.org/10.1111/cen.14276 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7361912/
16] Arvinte, C., Singh, M. & Marik, P. (18th Sept 2020 ). Serum Levels of Vitamin C and Vitamin D in a Cohort of Critically Ill COVID-19 Patients of a North American Community Hospital Intensive Care Unit in May 2020: A Pilot Study. Medicine in Drug Discovery Available online 18 September 2020, 100064 In Press, Uncorrected Proof https://doi.org/10.1016/j.medidd.2020.100064 Available at https://www.sciencedirect.com/science/article/pii/S2590098620300518?via%...
17] Baktash, V., Hosack, T., Patel, N., et al (27th August 2020 ). Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgraduate Medical Journal Published Online First: doi: 10.1136/postgradmedj-2020-138712 Available at https://pmj.bmj.com/content/early/2020/10/06/postgradmedj-2020-138712
18] Carpagnano, G., Di Lecce, V., Quaranta, N., Zito, A., Buonamico, E., Capozza, E., et al. (Aug 2020 ). Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J Endocrinol Invest. 2020 Aug 9:1–7. doi: 10.1007/s40618-020-01370-x. Available at https://pubmed.ncbi.nlm.nih.gov/32772324/
19] Cunat, T., Ojeda, A., & Calvo, A. (22 May 2020 ). Vitamin D deficiency in critically ill patients diagnosed with COVID -19. Are we doing enough? A retrospective analysis of 226 patients. Square Research. DOI: 10.21203/rs.3.rs-30390/v1 Available at https://www.researchsquare.com/article/rs-30390/v1
20] D'Avolio, A., Avataneo, V., Manca, A., Cusato, J., De Nicolò, A., Lucchini, R., Keller, F., & Cantù, M. (May 2020 ). 25-Hydroxyvitamin D Concentrations Are Lower in Patients with Positive PCR for SARS-CoV-2. Nutrients. 9;12(5):1359. doi: 10.3390/nu12051359. PMID: 32397511; PMCID: PMC7285131. Available at https://pubmed.ncbi.nlm.nih.gov/32397511/
21] De Smet, D., De Smet, K., Herroelen, P., Gryspeerdt, S., & Martens, G. ( 2020 ). Vitamin D deficiency as risk factor for severe COVID-19: a convergence of two pandemics. medRxiv; DOI: 10.1101/2020.05.01.20079376. Available from https://europepmc.org/article/ppr/ppr158640
22] Faniyi. A., Lugg. S., Faustini, S., Webster, C., Duffy, J., Hewison, M., et al. (6th October 2020 ). medRxiv 2020.10.05.20206706; doi: https://doi.org/10.1101/2020.10.05.20206706 Available at https://www.medrxiv.org/content/10.1101/2020.10.05.20206706v1
23] Fasano, A., Cereda, E., Barichella, M., Cassani, E., Ferri, V., Zecchinelli, L., & Pezzoli G. (Jul 2020 ) COVID-19 in Parkinson's Disease Patients Living in Lombardy, Italy. Mov Disord. 35(7):1089-1093. doi: 10.1002/mds.28176. Epub 2020 Jun 26. PMID: 32484584; PMCID: PMC7300944. Available From https://pubmed.ncbi.nlm.nih.gov/32484584/
24] Faul, J., Kerley, C., Love, B., O'Neill, E., Cody, C., et al. (7th May 2020 ). Vitamin D Deficiency and ARDS after SARS-CoV-2 Infection. Ir Med J. 2020 May 7;113(5):84. PMID: 32603575. Available from https://pubmed.ncbi.nlm.nih.gov/32603575/
25] Gennari, L., re by Robinson, K. (16th Sept 2020 ). Vitamin D Deficiency Is Independently Associated with COVID-19 Severity and Mortality. September 11. ASMBR 2020 Annual Meeting Virtual Event. Available at https://www.rheumatologynetwork.com/view/low-vitamin-d-may-worsen-covid-19
26] Ghasemian, R., Shamshirian, A., Heydari, K., Malekan, M., Alizadeh-Navaei, R., et al. (7th August 2020 ). The Role of Vitamin D in The Age of COVID-19: A Systematic Review and Meta-Analysis Along with an Ecological Approach. medRxiv 2020.06.05.20123554; doi: https://doi.org/10.1101/2020.06.05.20123554 Available from https://www.medrxiv.org/content/10.1101/2020.06.05.20123554v2
27] Kaufman, H., Niles, J., Kroll, M., Bi, C., & Holick, M. (17th Sept 2020 ). SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS One. 2020 Sep 17;15(9):e0239252. doi: 10.1371/journal.pone.0239252. PMID: 32941512; PMCID: PMC7498100. Available at https://pubmed.ncbi.nlm.nih.gov/32941512/
28] Im, H,. Je, Y., Baek, J., Chung, M., Kwon, H., & Lee, J. (11th Aug 2020 ). Nutritional status of patients with coronavirus disease 2019 (COVID-19), International Journal of Infectious Diseases, 2020, ISSN 1201-9712,
- https://doi.org/10.1016/j.ijid.2020.08.018.
- Available at http://www.sciencedirect.com/science/article/pii/S1201971220306470
29] Isaia, G. (25th March 2020 ) Possibile ruolo preventivo e terapeutico della vitamina D nella gestione della pandemia da COVID-19 Università degli Studi di Torino
30] Israel, A., Cicurel, A., Feldhamer, I., Dror, Y., Giveon, S., et al. (7th Sept 2020 ) The link between vitamin D deficiency and Covid-19 in a large population. medRxiv 2020.09.04.20188268; doi: https://doi.org/10.1101/2020.09.04.20188268 Available at https://journal.niidi.ru/jofin/article/view/1073/810https://www.medrxiv.... (In Russian)
31] Karahan, S., Katkat, F. (5th Oct 2020 ). Impact of Serum 25(OH) Vitamin D Level on Mortality in Patients with COVID-19 in Turkey. J Nutr Health Aging ( 2020 ). https://doi.org/10.1007/s12603-020-1479-0 Available at https://link.springer.com/article/10.1007/s12603-020-1479-0
32] Karonova, T., Andreeva, А., & Vashukova, М. ( 2020 ). Serum 25(oH)D level in patients with CoVID-19. Journal Infectology. 2020;12(3):21-27. https://doi.org/10.22625/2072-6732-2020-12-3-21-27 Available at
33] Kazaryan, A. re by Valera, D., (11th October 2020 ). UCSF Fresno study explores possible link between COVID-19 and Vitamin D. In the study, the majority of the patients with low Vitamin D levels landed in the ICU. YourCentralValley.com available at https://www.yourcentralvalley.com/news/ucsf-fresno-study-explores-possib...
34] Lau, F., Majumder, R., Torabi, R., Saeg, F., Hoffman, R., Cirillo, J., & Greiffenstein, P. (28th Apr 2020 ). Vitamin D Insufficiency is Prevalent in Severe COVID-19 doi: https://doi.org/10.1101/2020.04.24.20075838 Available from https://www.medrxiv.org/content/10.1101/2020.04.24.20075838v1
35] Macaya, F., Espejo, C., Valls, A., Fernández-Ortiz, A., del Castillo, J., et al. (20th July 2020 ). Interaction between age and vitamin D deficiency in severe COVID-19 infection. Hospital Clínico San Carlos. IdISSC. Universidad Complutense. Madrid, Spain 10.20960/nh.03193 Available at https://www.nutricionhospitalaria.org/articles/03193/show
36] Maghbooli, Z., Sahraian, M., Ebrahimi, M., Pazoki, M., Kafan, S., et al. ( 2020 ). Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PloS one, 15(9), e0239799. https://doi.org/10.1371/journal.pone.0239799 Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7518605/
37] Mardani, R., Alamdary, A., Mousavi Nasab, S., Gholami, R., Ahmadi, N., & Gholami, A. ( 2020 ). Association of vitamin D with the modulation of the disease severity in COVID-19. Virus Res. Aug 28;289:198148. doi: 10.1016/j.virusres.2020.198148. Epub ahead of print. PMID: 32866536; PMCID: PMC7455115. Available from https://pubmed.ncbi.nlm.nih.gov/32866536/
38] McCartney, D., & Byrne, D. (Apr 2020 ) Optimisation of Vitamin D Status for Enhanced Immuno-protection Against Covid-19. Ir Med J. 2020 Apr 3;113(4):58. PMID: 32268051. Available from https://pubmed.ncbi.nlm.nih.gov/32268051/
39] Meltzer, D., Best, T., Zhang, H., Vokes, T., Arora, V., & Solway, J. ( 2020 ). Association of Vitamin D Deficiency and Treatment with COVID-19 Incidence. medRxiv : the preprint server for health sciences, 2020.05.08.20095893. https://doi.org/10.1101/2020.05.08.20095893 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7274230/
40] Mendy, A., Apewokin, S., Wells, A. A., & Morrow, A. L. ( 2020 ). Factors Associated with Hospitalization and Disease Severity in a Racially and Ethnically Diverse Population of COVID-19 Patients. medRxiv : the preprint server for health sciences, 2020.06.25.20137323. https://doi.org/10.1101/2020.06.25.20137323 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7325178/
41] Merzon, E., Tworowski, D., Gorohovski, A., Vinker, S., Golan Cohen, A., Green, I., & Frenkel-Morgenstern, M. ( 2020 ). Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: an Israeli population-based study. The FEBS journal, 10.1111/febs.15495. Advance online publication. https://doi.org/10.1111/febs.15495 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7404739/
42] Philipose, Z., Smati, N., Wong, C., Aspey., & Mendall, M. (26th Aug 2020 ). Obesity, old age and frailty are the true risk factors for COVID-19 mortality and not chronic disease or ethnicity in Croydon. doi: https://doi.org/10.1101/2020.08.12.20156257
43] Pinzon, R., Angela, A., & Pradana, A. ( 2020 ). Vitamin D Deficiency Among Patients with COVID-19: Case Series and Recent Literature Review. Research Square; DOI: 10.21203/rs.3.rs-29473/v1. Available at https://europepmc.org/article/ppr/ppr165763
44] Pizzini, A., Aichner, M., Sahanic, S., Böhm, A., Egger, A., et. al. (Sept 2020 ) Impact of Vitamin D Deficiency on COVID-19-A Prospective Analysis from the CovILD Registry. Nutrients. Sep 11;12(9):E2775. doi: 10.3390/nu12092775. PMID: 32932831. Available at https://pubmed.ncbi.nlm.nih.gov/32932831/
45] Radujkovic, A., Hippchen, T., Tiwari-Heckler, S., Dreher, S., Boxberger, M., & Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. Available at https://www.mdpi.com/2072-6643/12/9/2757
46] Sun, J., Zhang, W., Zou, L., Liu, Y., Li, J, et. al. ( 2020 ). Serum calcium as a biomarker of clinical severity and prognosis in patients with coronavirus disease 2019. Aging, 12(12), 11287–11295. https://doi.org/10.18632/aging.103526 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7343468/
47] Silberstein, M. ( 2020 ). Correlation between premorbid IL-6 levels and COVID-19 mortality: Potential role for Vitamin D International Immunopharmacology Volume 88, November 2020, 106995 https://doi.org/10.1016/j.intimp.2020.106995 Available at https://www.sciencedirect.com/science/article/pii/S1567576920328976
48] Tort, A., Mercado, E., Martínez-Cuazitl, A., Nieto, A., & Pérez R. ( 2020 ). La deficiencia de vitamina D es un factor de riesgo de mortalidad en pacientes con COVID-19. (Deficiency of vitamin D is a risk factor of mortality in patients with COVID-19). Rev Sanid Milit Mex. 2020;74(1-2):. doi:10.35366/93773. Órgano de difusión del Servicio de Sanidad Militar y del Colegio Nacional de Médicos Militares. Available at https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=93773&idP...;
49] Yılmaz, K. and Şen, V. ( 2020 ). Is Vitamin D Deficiency a Risk Factor for Covid 19 in Children? Pediatric Pulmonology. Accepted Author Manuscript. doi:10.1002/ppul.25106 Available at https://onlinelibrary.wiley.com/doi/abs/10.1002/ppul.25106
50] Zanardi, M., De Carli, L., Ponta, M., & Pezzana, A. ( 2020 ). Nutritional approach to patients with coronavirus: Our experience in a 914 COVID-19-bed hospital. Nutrition (Burbank, Los Angeles County, Calif.), 110965. Advance online publication. https://doi.org/10.1016/j.nut.2020.110965 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7416677/
51] Alipio, M. (April 9, 2020 ). ‘Vitamin D Supplementation Could Possibly Improve Clinical Outcomes of Patients Infected with Coronavirus-2019 (COVID-19)’, SSRN. DOI: 10.2139/ssrn.3571484 Was available at https://ssrn.com/abstract=3571484 (Questions raised)
52] Glicio, El, J. (May 5, 2020 ). ‘Vitamin D Level of Mild and Severe Elderly Cases of COVID-19: A Preliminary Report’, SSRN. Previously available at: https://ssrn.com/abstract=3593258 (Questions raised)
53] Raharusun, P., Sadiah, P., Cahni, B., Erdie, A., Cipta, B. (April 26, 2020 ). ‘Patterns of COVID-19 Mortality and Vitamin D: An Indonesian Study’, SSRN. DOI: 10.2139/ssrn.3585561 Was available at: https://ssrn.com/abstract=3585561 (Questions raised)
54] Darling, A., Ahmadi, K., Ward, K., Harvey, N., Alves, A., Dunn-Waters, D., et. al. ( 2020 ). Vitamin D status, body mass index, ethnicity and COVID-19: initial analysis of the first-reported UK Biobank COVID-19 positive cases (n 580) compared with negative controls (n 723). medRxiv. 2020.04.29.20084277. doi: 10.1101/2020.04.29.20084277 Available at https://www.frontiersin.org/articles/10.3389/fpubh.2020.00513/full#B76
55] Hastie, C., Mackay, F., Ho, F., Celis-Morales, A., Katikireddi, V., Niedzwiedz, L., et al. ( 2020 ). Vitamin D concentrations and COVID-19 infection in UK Biobank. Diabetes Metab Syndrome Clin Res Rev. 14:561–5. doi: 10.1016/j.dsx.2020.04.050 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7204679/
56] Raisi-Estabragh, Z., McCracken, C., Bethell, M., Cooper, J., Cooper, C., Caulfield, J., et al. ( 2020 ). Greater risk of severe COVID-19 in non-White ethnicities is not explained by cardiometabolic, socioeconomic or behavioural factors, or by 25(OH)-vitamin D status: study of 1,326 cases from the UK Biobank. J Public Health. 42, 451–46 doi: 10.1093/pubmed/fdaa095/5859581. Available at https://academic.oup.com/jpubhealth/article/42/3/451/5859581
57] Fan, X., Wang, J., Song, M., Giovannucci, E., Ma, H., Jin, G., Hu, Z., Shen, H., & Hang, D. (July 4 2020 ). Vitamin D status and risk of all-cause and cause-specific mortality in a large cohort: results from the UK Biobank, The Journal of Clinical Endocrinology & Metabolism, dgaa432. https://doi.org/10.1210/clinem/dgaa432 Available at https://academic.oup.com/jcem/article/105/10/dgaa432/5867168
58] Fox, B., & Sizemore, J. No association seen between vitamin D deficiency and COVID-19 infection, hospitalization, or mortality. Epic Health Res. Netw ( 2020 ).
59] Tang, L., Liu, M., Ren, B., Wu, Z., Yu, X., Peng, C., Tian, J. (Aug. 2020 ). Sunlight ultraviolet radiation dose is negatively correlated with the percent positive of SARS-CoV-2 and four other common human coronaviruses in the U.S. Sci Total Environ. 19;751:141816. doi: 10.1016/j.scitotenv.2020.141816. Epub ahead of print. PMID: 32861186; PMCID: PMC7437529. Available at https://pubmed.ncbi.nlm.nih.gov/32861186/
60] Kohlmeier, M. (2009). Avoidance of vitamin D deficiency to slow the COVID-19 pandemic. BMJ Nutrition, Prevention & Health 2020;3: doi: 10.1136/bmjnph-2020-000096. Available at https://nutrition.bmj.com/content/3/1/67
61] Moan, J., Dahlback, A., Ma, L., & Juzeniene, A. (209). Influenza, solar radiation and vitamin D. Dermato-endocrinology, 1(6), 307–309. https://doi.org/10.4161/derm.1.6.11357 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3092571/
62] Juzeniene, A., Ma, L., Kwitniewski, M., Polev, G., Lagunova, Z., Dahlback, A., & Moan, J. (2010). The seasonality of pandemic and non-pandemic influenzas: the roles of solar radiation and vitamin D. Int J Infect Dis. 2010 Dec;14(12):e1099-105. doi: 10.1016/j.ijid.2010.09.002. Epub 2010 Oct 29. PMID: 21036090. Available at https://pubmed.ncbi.nlm.nih.gov/21036090/
63] Padhi, S., Suvankar, S., Panda, V., Pati, A., & Panda, A. ( 2020 ). Lower levels of vitamin D are associated with SARS-CoV-2 infection and mortality in the Indian population: An observational study. International Immunopharmacology, 88, 107001. https://doi.org/10.1016/j.intimp.2020.107001 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7489890/
64] Ilie, P., Stefanescu, S., Smith, L. (8th April 2020 ) The role of Vitamin D in the prevention of Coronavirus Disease 2019 infection and mortality. Square Research. Preprint. DOI:10.21203/rs.3.rs-21211/v1.
65] Mok, C., Ng, Y., Ahidjo, B., et al. ( 2020 ). Calcitriol, the active form of vitamin D, is a promising candidate for COVID-19 prophylaxis. bioRxiv; 2020. DOI: 10.1101/2020.06.21.162396. Available at https://europepmc.org/article/ppr/ppr179278
66] Biesalski H. K. ( 2020 ). Vitamin D deficiency and co-morbidities in COVID-19 patients – A fatal relationship? Nfs Journal, 20, 10–21. https://doi.org/10.1016/j.nfs.2020.06.001 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7276229/
67] Hanel, A., & Carlberg, C. ( 2020 ). ‘Vitamin D and evolution: Pharmacologic implications’, Biochem Pharmacol., 173(113595). DOI:10.1016/j.bcp.2019.07.024 Available at https://www.researchgate.net/publication/334851051VitaminDandevoluti...
68] Ramagopalan, S., Heger, A., Berlanga, A., et al. (2010). ‘A ChIP-seq defined genome-wide map of Vitamin D receptor binding: associations with disease and evolution’, Genome research, 20(10), p.1352–1360. DOI: 10.1101/gr.107920.110
69] Cooper, I., Crofts, C., DiNicolantonio. J., et al. ( 2020 ) Relationships between hyperinsulinaemia, magnesium, vitamin D, thrombosis and COVID-19: rationale for clinical management. Open Heart 2020;7:e001356. doi:10.1136/openhrt-2020-001356 Available at https://openheart.bmj.com/content/openhrt/7/2/e001356.full.pdf
70] Kuwabara, A., Tsugawa, N., Ao, M. Ohta, J., & Tanakac, K. (16 September 2020 ) Vitamin D deficiency as the risk of respiratory tract infections in the institutionalized elderly: A prospective 1-year cohort study Clinical Nutrition ESPEN https://doi.org/10.1016/j.clnesp.2020.08.012
71] Brenner, H., Holleczek, B., & Schöttker, B. ( 2020 ). Vitamin D Insufficiency and Deficiency and Mortality from Respiratory Diseases in a Cohort of Older Adults: Potential for Limiting the Death Toll during and beyond the COVID-19 Pandemic? Nutrients, 12(8), 2488. https://doi.org/10.3390/nu12082488 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7468980/
72] Grant, W., Lahore, H., McDonnell, S., Baggerly, C., French, C., Aliano, J., & Bhattoa, H. (30th March 2020 2nd version). Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients,12: 988. https://www.preprints.org/manuscript/202003.0235/v2
73] Brown, R., Sarkar, A. (29th Feb 2020 ). Vitamin D deficiency: a factor in COVID-19, progression, severity and mortality? – An urgent call for research. MitoFit Preprint Arch. doi:10.26124/mitofit:200001. https://www.mitofit.org/index.php/Brown2020MitoFitPreprintArch
74] Davies, G., Garami, A., & Byers, J. (13th June 2020 - also earlier versions). Evidence Supports a Causal Role for Vitamin D Status in COVID-19 Outcomes. medRxiv 2020.05.01.20087965; doi: https://doi.org/10.1101/2020.05.01.20087965 Available at: https://www.medrxiv.org/content/10.1101/2020.05.01.20087965v3.full.pdf (Accessed: 24 June 2020 ).
75] Benskin L. L. ( 2020 ). A Basic Review of the Preliminary Evidence That COVID-19 Risk and Severity Is Increased in Vitamin D Deficiency. Frontiers in public health, 8, 513. https://doi.org/10.3389/fpubh.2020.00513 Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7513835/
76] Brown, R. (April 7, 2020 ). Vitamin D deficiency; and, death rates; are both disproportionately higher in elderly Italians, Spanish, Swedish Somali, and African Americans? A connection? Research urgently required!’: ‘Rapid Response: Re: Preventing a covid-19 pandemic - COVID-19’: BMJ, 368(m810). DOI: 10.1136/bmj.m810 Available at https://www.bmj.com/content/368/bmj.m810/rr-46
77] Brown, R., Rhein, H., Alipio, M., Annweiler, C., Gnaiger, E., Holick M., Boucher, B., Duque, G., Feron, F., Kenny, R., Montero-Odasso, M., Minisola, M., Rhodes, J., Haq., A, Bejerot, S., Reiss, L., Zgaga, L., Crawford, M., Fricker, R., Cobbold, P., Lahore, H., Humble, M., Sarkar, A., Karras, S., Iglesias-Gonzalez, J., Gezen-Ak, D., Dursun E., Cooper, I., Grimes, D. & de Voil C. (April 20, 2020 ). COVID-19 ’ICU’ risk – 20-fold greater in the Vitamin D Deficient. BAME, African Americans, the Older, Institutionalised and Obese, are at greatest risk. Sun and ‘D’-supplementation – Game-changers? Research urgently required’: ‘Rapid response re: Is ethnicity linked to incidence or outcomes of COVID-19?’: BMJ, 369(m1548). DOI: 10.1136/bmj.m1548. Available at: https://www.bmj.com/content/369/bmj.m1548/rr-6 (Accessed: 24 June 2020 ).
78] Brown, R. (19th May 2020 ). ‘Low Vitamin D: high risk COVID-19 mortality? Seven preprints suggest that is case. Does low ‘D’ put BAME and elderly, at particular COVID-19 risk? Testing and Data Required’, BMJ, 369(m1548). DOI: 10.1136/bmj.m1548 Available at: https://www.bmj.com/content/369/bmj.m1548/rr-19.
79] Brown, R. (10th June 2020 ). ‘BAME Children at High Risk of PIMS-TS, a Covid-19 Kawasaki-Like Disease - Vitamin D, a Factor? – Testing and Data Urgently Required: Is ethnicity linked to incidence or outcomes of covid-19?’. BMJ, 369(m1548) DOI: 10.1136/bmj.m1548. Available at https://www.bmj.com/content/369/bmj.m1548/rr-25
80] Brown, R. (17th June 2020 ). ‘Is ethnicity linked to incidence or outcomes of covid-19? High BAME COVID-19 Mortality - Ethnicity a Factor? – Yet: Cardiovascular Disease – Hypertension – Diabetes - were rare in 1920-60’s in Indigenous Africans – Vitamin D an underrated factor?’, BMJ, 369(m1548). DOI: https://doi.org/10.1136/bmj.m1548 Available at: https://www.bmj.com/content/369/bmj.m1548/rr-26 (Accessed: 24 June 2020 ).
81] Brown, R. (25th June 2020 ). Pandemic - ‘Action This Day’ – Measure Vitamin D in COVID-19 Patients – Time is of Essence – BAME, Elderly and Obese are Disproportionately Dying. Covid-19: Public health agencies review whether vitamin D supplements could reduce risk. BMJ 2020;369:m2475 doi: https://doi.org/10.1136/bmj.m2475 (19th June 2020 ). Available at https://www.bmj.com/content/369/bmj.m2475/rr-1.
82] Brown, R. (24th July 2020 ) COVID-19 and Vitamin-D – NICE; Unthinking discrimination against BAME, Elderly and Obese? Affirmative-action needed to mitigate D deficiency, in high-COVID-risk groups: Covid-19: Public health agencies review whether vitamin D supplements could reduce risk. BMJ 2020;369:m2475 doi: https://doi.org/10.1136/bmj.m2475 (Published 19 June 2020 ) Available at https://www.bmj.com/content/369/bmj.m2475/rapid-responses
83] NICE (2018) Vitamin D deficiency in adults - treatment and prevention. Available at https://cks.nice.org.uk/topics/vitamin-d-deficiency-in-adults-treatment-...
84] McCullough, P., Amend, J., McCullough, W., Repas, S., Travers, J., & Lehrer, D. The Essential Role of Vitamin D in the Biosynthesis of Endogenous Antimicrobial Peptides May Explain Why Deficiency Increases Mortality Risk in COVID-19 Infections. Preprints 2020, 2020050265 (doi: 10.20944/preprints202005.0265.v1)..) Available at https://www.preprints.org/manuscript/202005.0265/v1
85] Annweiler, C., Hanotted, B., de l’Epreviere, C., Sabatier, J-M., Lafaie, L., & Célarier T. (13th Oct 2020 ). Vitamin D and survival in COVID-19 patients: A quasi-experimental study. The Journal of Steroid Biochemistry and Molecular Biology 13 October 2020, https://doi.org/10.1016/j.jsbmb.2020.105771 105771 Available at https://www.sciencedirect.com/science/article/pii/S096007602030296X
86] Ye, K., Tang, T., Liao, X., Shaw B., Deng, M., et. al. (13th Oct 2020 ) Does Serum Vitamin D Level Affect COVID-19 Infection and Its Severity? - A Case-Control Study. Journal of the American College of Nutrition. DOI: 10.1080/07315724.2020.1826005 Available at https://www.tandfonline.com/doi/full/10.1080/07315724.2020.1826005
See also in Vitamin D Life
COVID-19 treated by Vitamin D - studies, reports, videos
{include}
{include}
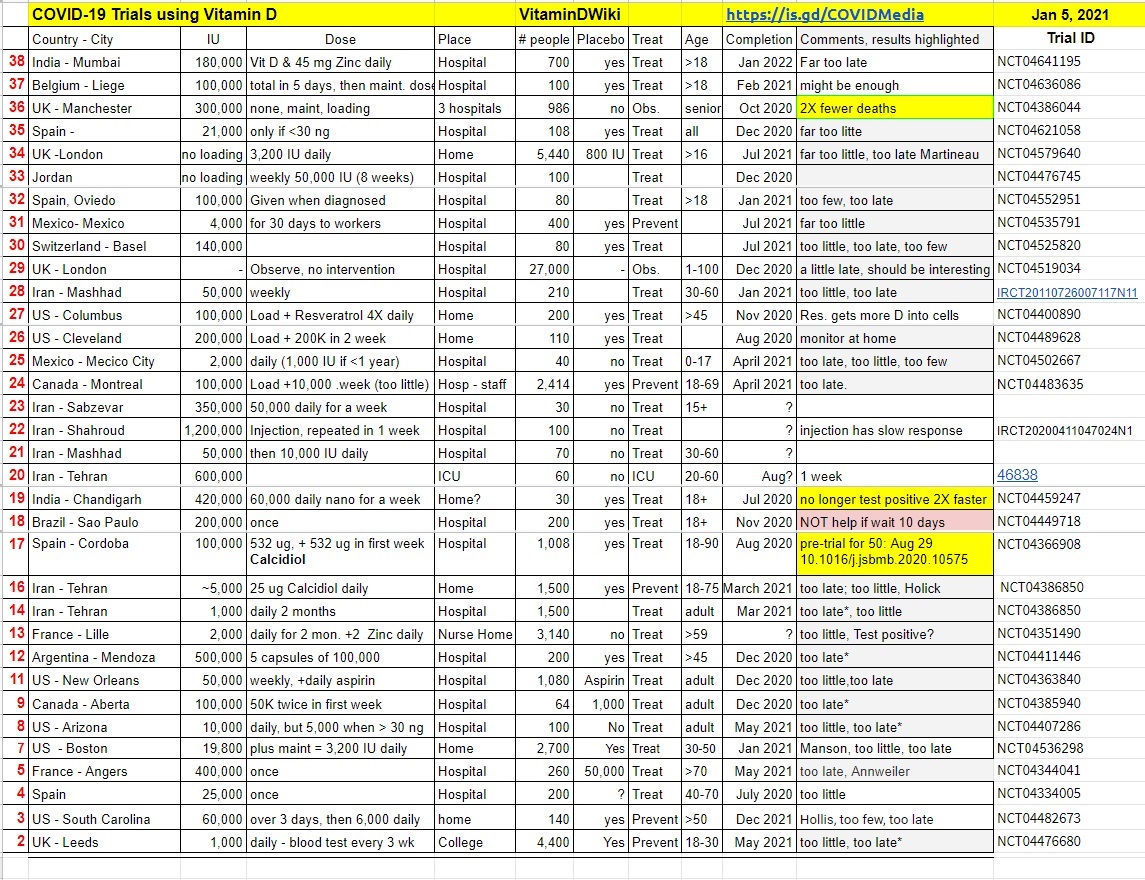
Many clinical trials are underway which are testing Vitamin D to fight COVID-19