Don’t be pregnant in Scotland
Vitamin D in pregnancy at high latitude in Scotland.
Br J Nutr. 2013 Mar 14;109(5):898-905. doi: 10.1017/S0007114512002255. Epub 2012 Jul 24.
Haggarty P, Campbell DM, Knox S, Horgan GW, Hoad G, Boulton E, McNeill G, Wallace AM.
Division of Lifelong Health, Rowett Institute of Nutrition and Health, University of Aberdeen, Greenburn Road, Bucksburn, Aberdeen AB21 9SB, UK.
Lowlights (definitely not highlights)
Only 21% of pregnant women supplement with vitamin D (median = 200 IU!)
< 1% of the pregnant women supplement with even 400 IU
Vitamin D levels of this very low supplementation resulted in no increase in the cord as birth
📄 Download the PDF from Vitamin D Life
Data from the article was made into a chart by Dr. Raimund von Helden
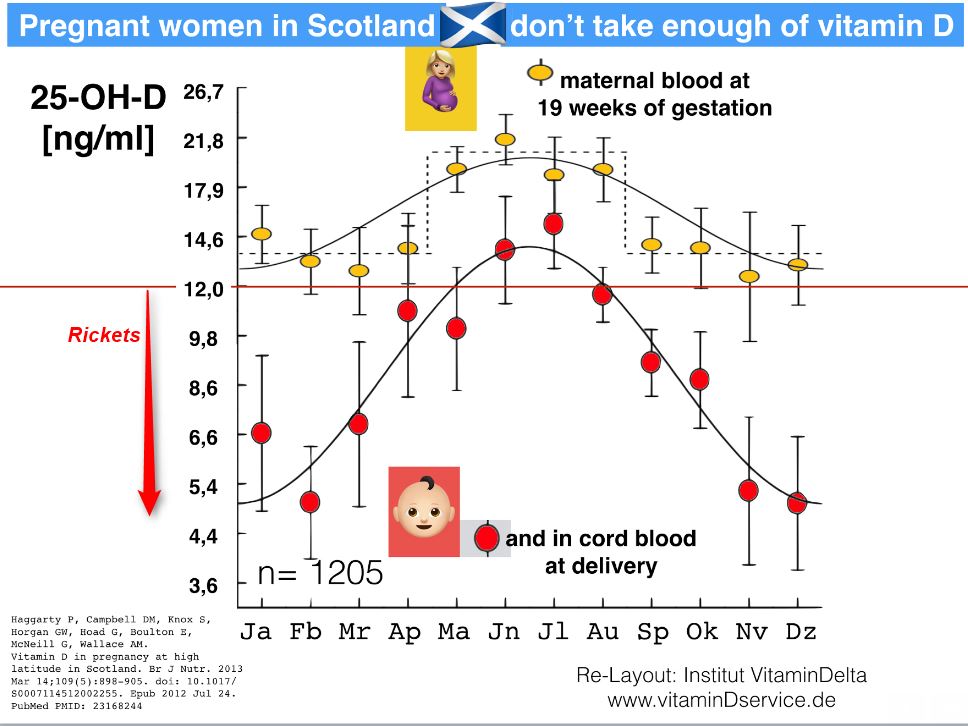
The aims of the present study were to determine compliance with current advice on vitamin D and to assess the influence of season, dietary intake, supplement use and deprivation on vitamin D status in pregnant mothers and newborns in the north of Scotland where sunlight exposure is low. Pregnant women (n 1205) and their singleton newborns were studied in the Aberdeen Maternity Hospital (latitude 57°N) between 2000 and 2006. Plasma 25-hydroxyvitamin D2 and 25-hydroxyvitamin D3 were measured at 19 weeks of gestation in mothers and at delivery in newborns. During pregnancy, 21·0 (95 % CI 18·5, 23·5) % of women took vitamin D supplements. The median intake was 5 μg/d and only 0·6 (95 % CI 0·1, 1·0) % took the recommended 10 μg/d. Supplement use, adjusted for season, dietary intake and deprivation, significantly increased maternal 25-hydroxyvitamin D (25(OH)D) by 10·5 (95 % CI 5·7, 15·2) nmol/l (P< 0·001); however, there was no significant effect on cord 25(OH)D (1·4 (95 % CI - 1·8, 4·5) nmol/l). The biggest influence on both maternal and cord 25(OH)D was season of birth (P< 0·001). Compared with the least deprived women (top three deciles), the most deprived pregnancies (bottom three deciles) were characterised by a significantly lower seasonally adjusted 25(OH)D ( - 11·6 (95 % CI - 7·5, - 15·7) nmol/l in the mother and - 5·8 (95 % CI - 2·3, - 9·4) nmol/l in the cord), and a lower level of supplement use (10 (95 % CI 4, 17) v. 23 (95 % CI 20, 26) %). More should be done to promote vitamin D supplement use in pregnancy but the critical importance of endogenous vitamin D synthesis, and known adaptations of fat metabolism specific to pregnancy, suggest that safe sun advice may be a useful additional strategy, even at high latitude.
PMID: 23168244
See also Vitamin D Life
UK pediatricians have a lot to learn about vitamin D – May 2012
A look at inner workings of committee looking at vitamin D for UK - Dec 2012
Chief UK Medical Officer recommends only 280 IU for children - Jan 2011
2X more preeclampsia when vitamin D less than 30 ng, etc. - meta-analysis March 2013
- Associated Editorial throws stones at UK policy of only 400 IU vitamin D during pregnancy
- 35,000 IU vitamin D weekly during 3rd quarter pregnancy – RCT March 2013
- Even 5,000 IU vitamin D daily was not enough
People with no UV for 6 months in the winter need at least 2000 IU of vitamin D – April 2011
Let 1000 die from vitamin D deficiency rather than incur 1 lawsuit