Is Vitamin D Supplementation Responsible for the Allergy Pandemic
Matthias Wjst
Posted: 05/22/2012; Curr Opin Allergy Clin Immunol. 2012;12(3):257-262. © 2012 Lippincott Williams & Wilkins
Matthias Wjst, Molecular Genetics of Lung Diseases, Comprehensive Pneumology Center (CPC), Institute of Lung Biology and Disease (iLBD), Helmholtz Zentrum München, German Research Center for Environmental Health, Ingolstädter Landstr. 1, D-85764 Neuherberg, Germany. E-mail: wjst@helmholtz-muenchen. de/[email protected]
(Impression after a very quick read by Vitamin D Life: Author speculates that low vitamin D during pregnancy sets up an expectation in the infant body for low vitamin D environment – which is upset by getting vitamin D. This would not occur if there were enough vitamin D during pregnancy)
CLICK HERE for original paper with reference numbers
Purpose of review A link between vitamin D supplementation and allergy was already suspected soon after it became possible to chemically synthesise vitamin D2 by means of ultraviolet radiation. During the past decade, the assumed allergenic effect was confirmed by clinical and epidemiological studies although the most recent discussion has centred more on vitamin D insufficiency. The purpose of this review is to summarise studies published during the past year while attempting to reconcile some apparent inconsistencies.
Recent findings Two new concepts are presented here – epigenetic programming of the fetal vitamin D system by low maternal vitamin D supply (Barker's paradox) and ubiquitous vitamin D exposure of the newborn (Rose's paradox). Taken together a misdirected epigenetic programming offers an explanation why also vitamin D insufficiency in pregnancy may be associated with increased allergy rates in the offspring.
At least eight studies examined the association of early 25-hydroxy-vitamin D levels and atopic diseases in 2011, whereas no new study addressed the question of vitamin D supplementation in the newborn period. One study tested the whole range of 25-hydroxy-vitamin D levels in cord blood describing a U-shaped association with 2.4-fold odds ratio of low and 4-fold odds ratio of high levels to develop allergen-specific immunoglobulin E.
Summary Randomised clinical trials with vitamin D supplements are therefore highly required. Several key points are presented for designing vitamin D trials.
Introduction
A supplement published by Nature in November 2011 summarised what allergy researchers currently know about the origins of the allergy epidemic: 'This […] is not a triumphant account of strategies that overcame allergy. Recent exploration of the complexities of the adaptive immune system has turned some assumptions about allergies upside down, and researchers are swimming in unfamiliar waters'.[1] This disillusioning view may be partially explained by the dominating hygiene hypothesis that could never been formulated as a true scientific hypothesis in a sense that it could be tested by a scientific method – either confirmed or refuted. It may be that real life circumstances do not follow formal logic. The situation from numerous observational studies in this area, however, is bizarre, most of them presenting a continuous flow of unconnected findings or arriving at contrary conclusions.
The interaction of the human adaptive immune system of 2 trillion lymphocytes is difficult to understand when it comes to the interaction with 100 trillion bacteria in the human gut or with the 1 quadrillion substances in the human environment. However, some progress appears to have been made in this area; a first interventional study[2] has shown that reduced helminthic load in pregnancy may prime allergy development in the offspring.
Historical Remarks
Only a small part of allergy research is currently dedicated to iatrogenic causes of the allergy epidemic. Nevertheless, it is a field of high potential in which we are dealing with clearly defined substances like micronutrients, vitamins, folate, antibiotics or paracetamol. A particularly interesting substance is vitamin D, used as a treatment for rickets since the 1920s. The substance has had a varied history until it was finally recommended by an European Union Directive in the 1990s as a baby food ingredient.[3] A link between vitamin D supplements and allergy was suspected as early as 1930 long before the modern vitamin D hypothesis was developed.[4] The rather speculative assumption in the 1990s was consecutively confirmed by clinical[5] and epidemiological studies[6,7] and mechanisms further elucidated by experimental data.[8] Vitamin D supplementation is unlikely to be the sole cause of the allergy pandemic but at least fair scientific evidence suggests that there is a risk for inducing allergy in the newborn.
The Vitamin D Insufficiency Discussion
Unexpectedly, however, vitamin D insufficiency[9,10] is now largely dominating the discussion.[11,12] Given the immunosuppressive function on respiratory infections this discussion is justified,[13] but it remains an unfortunate development with respect to allergy induction, in particular because this discussion is driven mainly by studies on serum levels of vitamin D that should not be confused with vitamin D supplement effects for several reasons.
First of all, serum 25-hydroxy-D3 level reflects a physiological state whereas vitamin D supplementation is being a nonphysiological action.
Second, serum 25-hydroxy-D3 measures a prohormone that is referred to as the nearly inactive storage form of vitamin D. The serum 25-hydroxy- D3 level is also subject to wide variation depending on race, sex, socioeconomic status and season.[14] The prohormone is obviously relevant only at extremely low and high levels. It can be safely assumed that a shortage of prohormone is not reached as long as we do not see any rickets symptoms.
Third, 25-hydroxy-vitamin D serum level is a poor proxy measurement of vitamin D effects as it is typically stored in fat tissue and acts as a nuclear hormone. The numerous studies of 25-hydroxy vitamin D serum levels have not been initiated because of the scientific value of this parameter but because of the easy access to blood samples and commercial kits.
Fourth, the serum 25-hydroxy vitamin D level is more a lifestyle than a biological marker.[15,16] Without an effective control of life circumstances influencing 25-hydroxy-D3 levels, there will be always an information bias and reverse confounding. Diseased individuals will avoid sun exposure[17] thus rendering most observational studies on 25-hydroxy-vitamin D levels uninformative.
Fifth, vitamin D insufficiency in general cannot be related to allergy prevalence as allergy was absent during the rickets epidemics that occurred in the last centuries.[3] There may be further allergy-inducing factors that act only in conjunction with low vitamin D status[13] although this has not been postulated so far.
Moreover, the discussion on the effects of vitamin D is becoming contentious possibly because of the complexity of the field. Studies are not cited correctly, vitamin D metabolites are not discriminated, or heavily biased towards beneficial effects of vitamin D.
Merging Two Old Concepts into a New One: Misdirected Epigenetic Programming
Before further summarising the studies on this topic published in 2011, two earlier concepts need to be introduced – Barker's early development[18] and Rose's smoking paradox[19] as both may help to understand the controversy around the vitamin D hypothesis.
David Barker pioneered the idea that the 20th century epidemic of coronary heart disease in Western countries might have originated in fetal life. Paradoxically, the epidemic coincided with improved standards of living and nutrition, yet in Britain its greatest impact was in the most deprived areas. Barker observed that early in the 20th century, these areas had the highest rates of neonatal mortality and by inference, the highest rates of low birth weight.[18] Based on that observation, Barker postulated that impaired fetal growth might have predisposed the survivors to heart disease in later life.
If we assume that early programming is a relevant factor for allergy as well (for example T-cell activation is already different at birth in allergy prone children),[20] maternal vitamin D levels may have an important function for presetting thresholds of vitamin D signalling and metabolism in the newborn. 25-hydroxy vitamin D crosses the placental barrier and 1,25-dihydroxy vitamin D is being largely synthesized in the fetus.[21] Effects may be simple induction or repression of genes of the cytochrome P450 superfamily that convert vitamin D metabolites,[22] a methylation of the vitamin D receptor itself[23] or by influencing various downstream interleukins.[24] Epigenetic decoupling of vitamin D feedback catabolism seems to play an important role in the placenta,[23] whereas it is becoming an important research question whether low maternal levels are ultimately leading to an upregulated vitamin D response in the newborn.
This may at least be expected from in-utero vitamin D-deficient mice that show a significant reduction in invariant NKT (iNKT) cell numbers that could not be corrected by later intervention with vitamin D.[25] Another example of in-utero priming of an allergic reaction has been shown by Hollingsworth who found multiple gene-associated loci, which were differentially methylated after in-utero supplementation with a methyl-rich diet.[26] These methylation changes were associated with decreased transcriptional activity and increased disease severity. It may be assumed that these are lasting effects by epigenetic cycles[27,28] explaining even more not very well understood phenomena.[27]
Rose's story is somewhat different[19] but equally important in that context. He considered two hypothetical populations in different settings. In the first setting, 50% are smokers, whereas in the second setting, 90% are smokers. If we assume an identical incidence of lung cancer in nonsmokers (two out of 100) and identical relative risks of 10, the proportion of population variation in lung cancer explained is 8.4% in the first, but, only 2.0% in the second setting. Even worse, in a third setting, wherein almost everyone smoked a pack of cigarettes a day, it would be impossible to find the real cause of lung cancer.
It is expected that ubiquitous supplement exposure of newborns – in analogy to the original Rose's paradox – will evoke a different reaction if a child has been raised in a low vitamin D intrauterine environment – in analogy to the original Barker paradox. Similar mechanisms have been described recently by the developmental origins of health and disease (DOHAD) movement that proposes that some disorders, such as type 2 diabetes and cardiovascular disease can result from an imbalance between the environments that are experienced in utero, in early infancy, and later life.[29] The Devereux[9] and Litonjua[10] studies in pregnant women therefore may have simply uncovered the higher sensitivity to the later supplement exposure – Vitamin Dtriggers and arms the immune system (Alleyne 2010). This sensitivity may be lost in later life as adults will adjust their vitamin D/calcium system to their own environment.[30]
The ubiquitous vitamin D exposure of all newborns in the Western world either by extra supplements or by general additive to baby food creates a great challenge for research. Effects will be extremely difficult to find in epidemiological studies – some studies may show effects with the dose of vitamin D.[6] Others with different pharmacological preparations of vitamin D[31] or gene variants related to vitamin D metabolism[32] or even show inverse associations[9] – this is what happened over the last decade in research on vitamin D and allergy.[13]
Vitamin D Studies in 2011
The final part of this review summarises human studies published in the last year relevant to vitamin D supplementation and the allergy pandemic (for effects of vitamin D in manifest diseases like asthma please refer to the accompanying article in this volume by Hollams). Due to space restraints, genetic studies are also not being reviewed here.
There were at least eight studies that examined vitamin D: van Oeffelen et al.;[33] Liu et al.;[34] Carroll et al.;[35] Hollams et al.;[36] Chi et al.;[37] Camargo et al.;[38] Morales et al. [39] and Rothers et al. [40] Unfortunately, none of these studies examined vitamin D supplement use in the newborn period. Four examined cord blood [34,37,38,40] and two, maternal blood. [35,39] The primary outcome in these studies was wheezing or asthma whereas only two studies reported allergic endpoints.[34,40]
Liu et al. [34] did not find an association of 25-hydroxy-vitamin D status with food sensitization. The study included 649 children who were enrolled at birth although vitamin D insufficiency was defined by cord blood levels less than 11 ng/ml, and food sensitization as specific IgE at least 0.35 kU/l to any of eight common food allergens. Only when examined jointly with SNPs in the IL4 gene was an association seen in which vitamin D insufficiency increased the risk of food sensitization among children carrying CC/CT genotypes[Odds ratio (OR) = 1.8, 95% confidence limit = 1.2–2.8].
The study of Chi et al. [37] provided many functional details from an inner-city birth cohort of 520 newborns who had at least one atopic parent. Umbilical cord plasma concentration of 25-hydroxy-vitamin D and the cytokine responses of cord blood mononuclear cells were compared under stimulation of phytohaemagglutinin, lipopolysaccharide and peptidoglycan. Most cytokine responses were not correlated with 25-hydroxyvitamin D concentration except a weakly positive association of IFNg release after lipopolysaccharide and a negative association with the proportions of CD25þ subset cells to total CD4þ T cells. As the suppressive activity of CD4þ25þ cells was not altered a clear picture did not emerge.
The study in New Zealand by Camargo et al. [38] solved a conundrum introduced by previous studies that did not distinguish between wheezing illness and asthma. In this new study, cord blood from 922 newborns was tested for 25-hydroxy-vitamin D and parents were asked if their child had a history of respiratory infection. As expected 25-hydroxyvitamin D had an inverse association with risk of wheezing by 3 months, 15 months, 3 years, and 5 years of age whereas no association with atopy or incident asthma was found.
In another study of the same group,[40] cord blood 25-hydroxy-vitamin D was measured in 219 children as well as specific IgE levels to six aeroallergens measured at age 1, 2, 3, and 5. Relative to the reference group both low (<50 nmol/l, P = 0.006) and high (?100nmol/l, P = 0.04) levels were associated with increased total immunoglobulin (Ig)E. Also allergen-specific IgE levels (OR = 2.4, P = 0.03 and OR = 4.0, P = 0.01, respectively) were increased; however, no association with allergic rhinitis or asthma was found. This is interesting because such a U-shaped relationship has also been found also in our own[41] but also other studies.[42]
Conclusion
To solve these vexing questions, we probably need a shift in research priorities[43] away from observational studies and study parameters of limited use. The plethora of positive associations of serum 25-hydroxy-vitamin D and cardiovascular disease have only recently been decided by a controlled trial.[44] We probably do not need any further observational studies in allergy research but randomized clinical trials of vitamin D supplements, starting in pregnancy and extending over the newborn period with final outcomes measured at later ages (Fig. 1). There are also numerous biological readouts that could accompany those trials to identify biological pathways using DNA methylation, gene expression pattern or proteomics data from relevant cell subsets. Such trials could ultimately show everything about vitamin D[45] to get the most benefit for the health of our children.
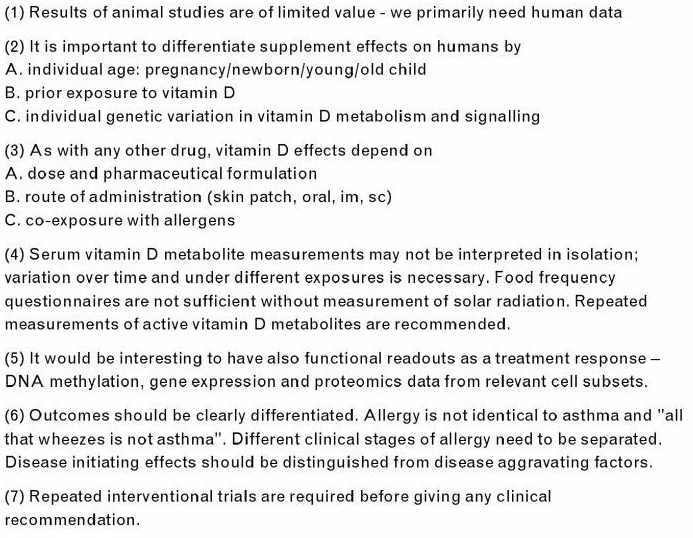
Figure 1. Vitamin D study design issues. To solve the most controversial issue surrounding vitamin D effects on allergy and asthma, several key points may be considered.
Key Points
A link between vitamin D supplementation and allergy was already suspected soon after it became possible to chemically synthesise vitamin D.
Both vitamin D insufficiency and vitamin D supplementation have been linked to allergy and asthma. This apparent paradox is explained by epigenetic programming in pregnancy by low vitamin D levels and the excessive high supplementation in the newborn period.
The current literature is being reviewed, showing no new study that addressed the question of vitamin D supplementation in the newborn period. We conclude that randomised clinical trials are therefore urgently required.
References (have to CLICK HERE to see the original paper with the reference numbers)
East R. Allergies. Nature 2011; 479:S1.
- Most recent and comprehensive lay description on current allergy research. Unfortunately, the supplement missed a discussion of iatrogenic origins.
Mpairwe H, Webb EL, Muhangi L, et al. Anthelminthic treatment during pregnancy is associated with increased risk of infantile eczema: randomised-controlled trial results. Pediatr Allergy Immunol 2011; 22:305–312.
Wjst M. Introduction of oral vitamin D supplementation and the rise of the allergy pandemic. Allergy Asthma Clin Immunol 2009; 5:5–8.
Wjst M, Dold S. Genes, factor X, and allergens: what causes allergic diseases? Allergy 1999; 54:757–759.
Moneret-Vautrin DAHR, Kanny G, Ait-Djafer Z. Allergenic peanut oil in milk formulas. Lancet 1991; 338:1149.
Hyppönen E, Sovio U, Wjst M, et al. Vitamin D supplementation in infancy and the risk of allergies in adulthood: a birth cohort study. Ann Am Acad Sci 2004; 1037:84–95.
Milner JD, Stein DM, McCarter R, Moon RY. Early infant multivitamin supplementation is associated with increased risk for food allergy and asthma. Pediatrics 2004; 114:27–32.
Matheu V, Bäck O, Mondoc E, Issazadeh-Navikas S. Dual effects of vitamin Dinduced alteration of TH1/TH2 cytokine expression: enhancing IgE production and decreasing airway eosinophilia in murine allergic airway disease. J Allergy Clin Immunol 2003; 112:585–592.
Devereux G, Litonjua AA, Turner SW, et al. Maternal vitamin D intake during pregnancy and early childhood wheezing. Am J Clin Nutr 2007; 85:853– 859.
Litonjua AA, Rifas-Shiman SL, Ly NP, et al. Maternal antioxidant intake in pregnancy and wheezing illnesses in children at 2 y of age. Am J Clin Nutr 2006; 84:903–911.
Benson AA, Toh JA, Vernon N, Jariwala SP. The role of vitamin D in the immunopathogenesis of allergic skin diseases. Allergy 2012; 67:296– 301.
Weiss ST. Bacterial components plus vitamin D: the ultimate solution to the asthma (autoimmune disease) epidemic? J Allergy Clin Immunol 2011; 127:1128–1130.
Wjst M. The vitamin D slant on allergy. Pediatr Allergy Immunol 2006; 17:477–483.
Arguelles LM, Langman CB, Ariza AJ, et al. Heritability and environmental factors affecting vitamin D status in rural Chinese adolescent Twins. J Clin Endocrinol Metab 2009; 1–25.
Grimes DS. Vitamin D and the social aspects of disease. QJM 2011; 104:1065–1074.
Tsiaras WG, Weinstock MA. Factors influencing vitamin D status. Acta Dermato-Venereologica 2011; 91:115–124.
Arnedo-Pena A, García-Marcos L, Fernández-Espinar JF, et al. Sunny hours and variations in the prevalence of asthma in schoolchildren according to the International Study of Asthma and Allergies (ISAAC) Phase III in Spain. Int J Biometeorol 2011; 55:423–434.
Robinson R. The fetal origins of adult disease. BMJ 2001; 322:375– 376.
Pearce N. Epidemiology in a changing world: variation, causation and ubiquitous risk factors. Int J Epidemiol 2011; 40:503–512.
- This is a background article relevant to understand many phenomena of current research.
Martino DJ, Bosco A, McKenna KL, et al. T-cell activation genes differentially expressed at birth in CD4(þ) T-cells from children who develop IgE food allergy. Allergy (in press).
- Although the sample was rather small the study identifies transient, suboptimal neonatal T-cell activation pathways that signal through the NF-kB complex and postulates that these may increase the risk of food allergy.
Ponsonby A-L, Lucas RM, Lewis S, Halliday J. Vitamin D status during pregnancy and aspects of offspring health. Nutrients 2010; 2:389–407.
Marik R, Fackler M, Gabrielson E, et al. DNA methylation-related vitamin D receptor insensitivity in breast cancer. Cancer Biol Therapy 2010; 10:44–53.
Novakovic B, Sibson M, Ng HK, et al. Placenta-specific methylation of the vitamin D 24-hydroxylase gene: implications for feedback autoregulation of active vitamin D levels at the fetomaternal interface. J Biol Chem 2009; 284:14838–14848.
Wessels I, Fleischer D, Rink L, Uciechowski P. Changes in chromatin structure and methylation of the human interleukin-1ß gene during monopoiesis. Immunology 2010; 130:410–417.
Yu S, Cantorna MT. Epigenetic reduction in invariant NKT cells following in utero vitamin D deficiency in mice. J Immunol 2011; 186:1384–1390.
- The article presents a key finding given the importance of iNKT cells for allergy. Vitamin D deficiency-induced reduction in iNKT cells is most likely because of increased apoptosis of early iNKT cell precursors in the thymus.
Hollingsworth JW, Maruoka S, Boon K, et al. In utero supplementation with methyl donors enhances allergic airway disease in mice. J Clin Investigation 2008; 118:3462–3469.
Gabory A, Attig L, Junien C. Developmental programming and epigenetics. Am J Clin Nutr 2011; 94:1943S–1952S.
Gallou-Kabani C, Vige A, Gross MS, Junien C. Nutri-epigenomics: lifelong remodelling of our epigenomes by nutritional and metabolic factors and beyond. CCLM/FESCC 2007; 45:321–327.
Hochberg Z, Feil R, Constancia M, et al. Child health, developmental plasticity, and epigenetic programming. Endocrine Rev 2011; 32:159–224.
- This is an excellent article summarizing our current knowledge on programming and misadaptation to environmental conditions.
Sharief S, Jariwala S, Kumar J, et al. Vitamin D levels and food and environmental allergies in the United States: results from the National Health and Nutrition Examination Survey. J Allergy Clin Immunol 2005–2006; 127:1195– 1202.
Kull I, Bergstrom A, Melen E, et al. Early-life supplementation of vitamins A and D, in water-soluble form or in peanut oil, and allergic diseases during childhood. J Allergy Clin Immunol 2006; 118:1299–1304.
Raby BA, Lazarus R, Silverman EK, et al. Association of vitamin D receptor gene polymorphisms with childhood and adult asthma. Am J Respir Crit Care Med 2004; 170:1057–1065.
Van Oeffelen AAM, Bekkers MBM, Smit HA, et al. Serum micronutrient concentrations and childhood asthma: the PIAMA birth cohort study. Pediatr Allergy Immunol (in press).
Liu X, Wang G, Hong X, et al. Gene-vitamin D interactions on food sensitization: a prospective birth cohort study. Allergy 2011; 66:1442–1448.
Carroll KN, Gebretsadik T, Larkin EK, et al. Relationship of maternal vitamin D level with maternal and infant respiratory disease. Am J Obstet Gynecol 2011; 205:215.
Hollams EM, Hart PH, Holt BJ, et al. Vitamin D and atopy and asthma phenotypes in children: a longitudinal cohort study. Eur Respir J 2011; 38:1320–1327.
Chi A, Wildfire J, Mcloughlin R, et al. Umbilical cord plasma 25-hydroxyvitamin D concentration and immune function at birth: the Urban Environment and Childhood Asthma study. Clin Exp Allergy 2011; 41:842–850.
Camargo CA, Ingham T, Wickens K, et al. Cord-blood 25-hydroxyvitamin D levels and risk of respiratory infection, wheezing, and asthma. Pediatrics 2011; 127:e180–e187.
- This article clarifies an important issue – vitamin D is associated with a lower frequency of respiratory infections but not of asthma.
Morales E, Romieu I, Guerra S, et al. Maternal vitamin D status in pregnancy and risk of lower respiratory tract infections, wheezing, and asthma in offspring. Epidemiology (in press).
Rothers J, Wright AL, Stern DA, et al. Cord blood 25-hydroxyvitamin D levels are associated with aeroallergen sensitization in children from Tucson, Arizona. J Allergy Clin Immunol 2011; 128:1093–1099.
- This is careful conducted and analysed study showing a U-shaped association of 25-hydroxy-vitamin D serum level and IgE.
Hypponen E, Berry DJ, Wjst M, Power C. Serum 25-hydroxyvitamin D and IgE: a significant but nonlinear relationship. Allergy 2009; 64:613–620.
Ross AC, Manson JE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab 2011; 96:53–58.
Willyard C. Drug developers explore vitamin D benefits without the vitamin. Nat Med 2011; 17:9.
Avenell A, Maclennan GS, Jenkinson DJ, et al. Long-term follow-up for mortality and cancer in a randomized placebo-controlled trial of vitamin D3 and/or calcium (RECORD trial). J Clin Endocrinol Metab (in press).
Cannell JJ. The difference between a prophet and a madman. Br J Nutr 2011; 106:1317–1318.
Papers of particular interest, published within the annual period of review, have been highlighted as:
of special interest
- of outstanding interest
Acknowledgements
I wish to thank Carol Oberschmidt (Berlin) and Loems Ziegler-Heitbrock (Gauting) for a critical revision of the manuscript, Rasso Ranzinger (München) for providing the literature as well as many colleagues for invitations and helpful discussions over the past years: Elina Hyppö- nen (London), Carlos Camargo (Boston), John Mc Grath (Brisbane), Graham Devereux (Aberdeen), Sunit Jariwala (New York), Eduardo Egea (Barranquilla), Merete Jorgensen (Copenhagen), Talat Islam (Los Angeles), Susanne Krauss-Etschmann (München), Tania Sih (Sao Paulo) and Seif Shaheen (London). I further want to thank the American Academy of Allergy, Asthma and Immunology for their travel grants while there was no particular funding of the work presented here.