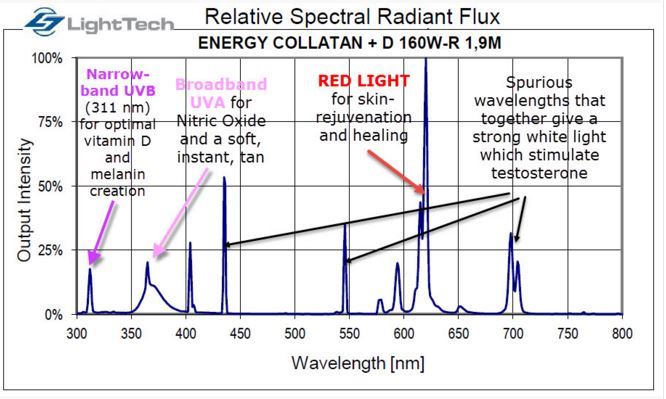
Many wavelengths of light provide health benefits, not just UV
Biological Effects of Sunlight, Ultraviolet Radiation, Visible Light, Infrared Radiation and Vitamin D for Health
ANTICANCER RESEARCH 36: 1345-1356 (2016)
MICHAEL F. HOLICK, Section of Endocrinology, Diabetes and Nutrition, Department of Medicine, Boston University Medical Center, 85 East Newton St., Boston, MA 02118, U.S.A. [email protected]
Abstract. Humans evolved in sunlight and had depended on sunlight for its life giving properties that was appreciated by our early ancestors. However, for more than 40 years the lay press and various medical and dermatology associations have denounced sun exposure because of its association with increased risk for skin cancer. The goal of this review is to put into perspective the many health benefits that have been associated with exposure to sunlight, ultraviolet A (UVA) ultraviolet B (UVB), visible and infrared radiation.
📄 Download the PDF from Vitamin D Life
Historical Perspective
The earth has been bathing in sunlight for more than 3 billion years. As life forms evolved in the ocean they were exposed to sunlight. The energy from the sun was efficiently utilized by early phytoplankton to produce carbohydrates as their energy source. However exposure to the sunlight had some negative consequences. The ultraviolet B (UVB) radiation that penetrated through the atmosphere was absorbed by photosensitive macromolecules including proteins, RNA and DNA in these unicellular organisms that resulted in alterations in their structure. As a result mechanisms evolved to repair the structural defects induced by absorbing this energy during sun exposure. Furthermore, organisms also likely evolved sunscreens to efficiently absorb the UVB radiation in the plasma membrane, thereby reducing the number of photons reaching the photosensitive macromolecules within the cell. Ergosterol would have served as an excellent sunscreen since it has an absorption spectrum that spans wavelengths from approximately 240-315 nm. When ergosterol absorbs UVB radiation its energy is dissipated by the re-arrangement of the double bonds in the B ring causing the cleavage of the bond between carbons 9-10. This cleavage results in an opening of the B-ring forming previtamin D2. Previtamin D2 has a UV absorption spectrum that is essentially identical to DNA and RNA with a peak absorption at 260 nm and thus also served as a sunscreen protecting the genetic material within the cell from the damaging UVB radiation. Previtamin D2 however is thermodynamically unstable and it undergoes a rearrangement of its 3 double bonds, forming the more stable vitamin D2. Vitamin D2, similar to previtamin D2, has a UV absorption spectrum similar to DNA and RNA with a peak absorption at 265 nm. The planar structure of cis-cis- previtamin D2 which was sandwiched in between the hydrocarbon side chains becomes disrupted as it undergoes its transformation to the 5, 6-cis-vitamin D2. As a result of this structural transformation vitamin D2 is ejected from the plasma membrane either intracellularly or extracellularly. This likely resulted in a transient opening of the plasma membrane permitting the transit of calcium into and out of the cell. Thus the intimate connection between sunlight- vitamin D and calcium was born (1, 2).
Sunlight Energy and the Skin
The sun produces an enormous amount of energy including cosmic, gamma rays, x-rays, UVB and UVA radiation, visible radiation and infrared radiation. All of the high-energy cosmic, gamma and x-radiation are reflected or absorbed by the atmosphere that envelops our planet. Most of the UV radiation is efficiently absorbed by the stratospheric ozone layer. All UVC (200-280 nm) radiation is efficiently absorbed by the ozone layer and none reaches the earth’s surface. Most of the UVB radiation (290-320) nm is absorbed by the ozone layer. Approximately 0.1% reaches the earth surface at noon time at the equator in the summer. Approximately 5% of UVA radiation (321-400 nm) reaches earth surface. A larger fraction of visible radiation (39%) and infrared radiation (56%) reaches the earth’s surface (Figure 1).
There is an inverse relationship between wavelength and energy. Lower wavelengths of radiation have higher energy.
When human skin is exposed to sunlight it would be reasonable to conclude that the highest energy radiation i.e. UVB radiation would penetrate more deeply into the skin than lower energy photons such as UVA and visible radiation. However the skin contains a variety of macromolecules including RNA, DNA and proteins that efficiently absorb UVB photons and therefore almost all of the UVB photons are absorbed by the macromolecules in the epidermis. These macromolecules are less efficient in absorbing UVA radiation and as a result UVA radiation penetrates through the epidermis into the dermis. Very little visible and infrared radiation is absorbed by the epidermis or dermis and thus can penetrate deep into the body cavity bathing internal organs (Figure 2A). In response to exposure to sunlight, skin responds by increasing the amount of the upper dead layer, the stratum corneum, which act like mirrors and reflect and refract UVA and UVB radiation. The UVA and UVB radiation that penetrates through the epidermis reaching the epidermal-dermal junction are absorbed by the melanocytes inducing them to produce melanin (Figure 2B). The melanin is packaged into melanosomes that are released into the epidermis where they settle over the nuclei of the epidermal cells acting as an umbrella to absorb the UVB and UVA radiation so that they do not enter the cell. Absorption of UVA radiation in the epidermis and dermis can cause the formation of free radicals which can damage proteins, DNA and RNA in the cells (3). Besides being an extremely efficient sunscreen, melanin, also acts as an antioxidant and free radical scavenger, thereby reducing free radical damage to the cells (4).
Sunlight , Skin Cancer, Wrinkles and the Immune System
When DNA absorbs UV radiation this can cause cross linking of the pyrimidine bases, thymine and cytosine. Double-stranded RNA can also form uracil dimers (5). The two common UVB products are cyclo-butane pyrimidine dimers and 6,4-pryimidine-pyrimidones. These premutagenic lesions alter the structure of DNA and consequently inhibit DNA polymerases and arrest cell replication (6, 7). These dimers are usually repaired by photoreactivation or nucleotide excision repair (8-10). The unrepaired dimers are mutagenic. It is believed that certain genes such as the p53 tumor suppressor gene if unrepaired can lead to unregulated hyper-proliferation of the epidermal cell causing an actinic keratosis. If both p53 genes are affected this can lead to nonmelanoma squamous cell skin cancer (11).
Melanoma being the most deadly skin cancer is often found on the least sun-exposed areas. Risk factors for melanoma include number of sun burn experiences as a child and young adult, genetic predisposition, red hair color, increased numbers of moles on the body. Occupational sun exposure has been associated with a reduced risk for this deadly skin cancer (12).
Response of thickened, pigmented epidermis to UV radiation
Figure 2 . A. Penetration of ultraviolet B (UVB), ultraviolet A (UVA), visible and infrared radiation in the human skin. B. In response to exposure to UVB and UVA radiation the stratum corneum thickens and melanocytes at the epidermal-dermal junction are stimulated to produce melanin. (With permission Holick copyright 2016).
UVA radiation creates free radicals that can also damage the DNA in skin cells increasing the risk for malignancy (13). In addition UVA that penetrates into the dermis can cause cross-linking of the collagen-elastin network resulting in skin damage and wrinkling (14). It also has an effect on the immune system increasing immune tolerance (Figure 3) (15).
Historical Perspective and Health Consequences of Sunlight Deprivation
In the early 19th century most scientists believed that the only effect of sunlight on the skin was to generate heat, which was responsible for sun burning. However Dr. E. Holmes conducted a simple study where he exposed one hand to sunlight and at the same time measured the temperature of the surrounding air for a period of time that caused the erythema, blistering and pain.
Figure 3. Exposure to sunlight results in a variety of responses in the skin. (With permission Holick copyright 2016).
He recorded the air temperature to be 90°F. At the same time he exposed the other hand to sunlight that had a cloth placed above the hand. This hand did not experience any erythema, blistering or pain even though the temperature was found to be 102°F. He also exposed a black Granadian’s hand the same amount of sunlight and demonstrated that the skin pigmentation prevented the skin from being sun burned (16).
This was the first demonstration that sunlight itself penetrating into white skin had a biological effect and that skin pigmentation was a “defense against scorching effects of the sun”.
As the industrial revolution swept across Northern Europe in the late 17th century physicians began reporting that children living in the inner cities of Glasgow and London were developing skeletal deformities especially prominent in the legs as well as growth retardation. By the turn of the 19th century it was estimated that more than 90% of children living in the industrial cities throughout Europe had this bone deformity disease known as rickets (17). In 1822 Sniadecki reported that children living in Warsaw were afflicted with rickets whereas children living in the rural areas outside of Warsaw did not develop this bone deformity disease. He concluded “strong and obvious is the influence of sun on the cure of rickets and the frequent occurrence of the disease in densely populated towns where the streets are narrow and poorly lit” (18). It was inconceivable to the medical community how exposure of the skin to sunlight could have any health consequences on the skeleton and this observation was ignored for almost 100 years. In 1889 Palm wrote to his colleagues, living in India and china where nutrition was extremely poor and children lived in squalor, asking whether they were seeing children with rickets. They reported back that it was a rare condition. He reasoned that children living in London had better nutrition and better housing conditions and therefore the only common denominator was that children living in the polluted cities of London and Glasgow were not exposed to any sunlight. He encouraged sunbathing as a method to treat and prevent rickets (19).
At the same time Finsen was using sunlight in its various forms to treat lupus vulgaris, a skin disease caused by tuberculosis infection. For his insightful observations he received the Nobel Prize in 1903 (20).
In 1919 Huldschinsky reported that children exposed to a mercury arc lamp was an effective treatment for rickets (21). This was quickly followed by the report of Hess and Unger (22) that exposure of children with rickets to sunlight was effective in treating this bone disease. These observations were quickly translated into the practice of irradiating food with UV radiation that imparted anti-rachitic activity (23). Ergosterol, produced by yeast, when exposed to UVB radiation had anti-rachitic activity and the factor was identified eventually as vitamin D2. Milk was initially fortified with ergosterol followed by UV irradiation to impart anti-rachitic activity. When vitamin D2 was commercially produced it was simply added to the milk. This simple process was effective in essentially eliminating this bone disease as a health issue in countries that used this fortification practice.
It was quickly realized that the skin when exposed to sunlight made a different vitamin D. It was identified as vitamin D3. It was produced from a precursor of cholesterol, 7- dehydrocholesterol by Windaus et al. (26). For his discoveries of vitamin D3 he received the Nobel Prize in 1928.
These observations prompted a revolution in thinking on the health benefits of sunlight and gave rise to the concept of heliotherapy. In the early 1930s the United States government sent out a brochure to parents encouraging sunbathing for their infants to “help him grow normally”. The brochure also noted that “dark-skinned babies need more sun to protect them from rickets than fair-skinned babies.”
Thus sunlight exposure was encouraged for good health and vitamin D was fortified in a wide variety of products including not only milk and bread but also custard, soda pop, hotdogs and beer (16).
In the late 1940s and early 1950s very high doses of vitamin D given to infants resulted in them developing hypercalcemia (25). In addition there were reports from Great Britain of infants who had altered facial structure, heart problems, mental retardation and hypercalcemia. It was concluded by the experts from the Royal College of Physicians and the British Pediatric Association that this was caused by vitamin D intoxication presumably due to overfortification of milk with vitamin D. As a result Great Britain passed laws banning the fortification of any product including foodstuffs and even topical skin creams from being fortified with vitamin D. The hysteria that vitamin D at high doses could cause birth defects and mental retardation spread throughout Europe and most of the world and as a result most countries of the world today still do not permit the fortification of even milk with vitamin D. In retrospect it’s likely that these infants had a William’s syndrome (26). This rare genetic disorder is associated with elfin faces, heart problems, mild mental retardation and have a hypersensitivity to vitamin D that can cause hypercalcemia (26, 27).
Unfortunately to this day most health care professionals are taught that vitamin D is one of the most toxic fat-soluble vitamins and continues to be tightly regulated by health officials in government agencies.
Sunlight and Vitamin D
The major source of vitamin D for most children and adults is exposure to sunlight (17, 28). Very few foods naturally contain vitamin D; they include wild caught salmon, other oily fish, cod liver oil and sun-dried mushrooms (28). Some countries including the United States, Canada and Sweden encouraged the fortification of milk with vitamin D. Many countries fortify margarine with vitamin D.
During sun exposure UVB radiation with wavelengths of 290-315 nm are absorbed by 7-dehydrocholesterol in the plasma membrane of epidermal cells resulting in production of cis,cis-previtamin D3 (1, 2). This thermodynamically unstable molecule within the plasma membrane begins to rapidly isomerize by a non-enzymatic membrane-enhanced process within a few hours to vitamin D3. Once formed, vitamin D3 exits the circulation and is transported to the liver where it is converted to 25-hydroxyvitamin D3 [25(OH)D] (28, 29). This is the major circulating form of vitamin D, which is measured by physicians, to determine a person’s vitamin D status. However 25(OH)D has little biological activity and travels to the kidneys where it is converted to its active form, 1,25-dihydroxyvitamin D [1,25(OH)2D]. Once formed 1,25(OH D travels to the small intestine to increase in intestinal calcium absorption and to the skeleton to mobilize calcium when there is an inadequate amount of calcium coming from the diet (Figure 4) (28, 29).
Many tissues and cells in the body including macrophages, brain, breast, prostate, colon and skin, to name a few, have the capacity to convert 25(OH)D to 1,25(OH D (29, 30). These cells also have a vitamin D receptor (VDR) and once formed in the cell 1,25(OH)2D interacts with its nuclear receptor to unlock genetic information that controls numerous metabolic processes including DNA repair, antioxidant activity and regulating cellular proliferation and differentiation (Figure 4) (31, 32).
Influence of UVB, UVA and Visible Radiation on the Cutaneous POMC, Biologic Clock Genes and Melatonin Production
People have a feeling of well-being when exposed to sunlight. When cultured human keratinocytes were exposed to UVA or UVB and UVA radiation the cells exposed to UVA and UVB radiation had a marked increase in the expression and production of beta-endorphin compared to cells exposed only to UVA radiation (Figure 3) (33). Skin biopsies of adults exposed to UVB radiation demonstrated increased expression of beta endorphin in the keratinocytes (34). Healthy adults exposed to a tanning bed were reported to increase serum beta-endorphin levels by 44% (35). Beta- endorphin, an endogenous opioid peptide, has been demonstrated to improve not only feeling of wellbeing i.e. runners high, but also can cause pain relief and relaxation. Sunlight deprivation is associated with depression. In the winter this can cause, for those who are susceptible, seasonal affective disorder (SAD). Our circadian rhythm is controlled by blue light being absorbed by photoreceptors in the eye resulting in a decrease in melatonin production (36). For some people the decrease in the intensity of sunlight affected by seasonal changes prevents the suppression of melatonin and as a result the person wants to sleep and becomes listless and depressed. Bright-light therapy with 10,000 lumens for 30 min to 1 h in the morning can help suppress melatonin production in the pineal gland, thereby relieving many of the symptoms associated with SAD (37, 38).
it is now recognized that all cells express genes that are able to keep cellular time. It was demonstrated that these clock genes express transcription factors that regulate gene expression activity and thereby keep time in the various cells.
A good example was a report that most cells in a fruit fly express these clock genes (39). It was observed that the period (PER) gene appeared and disappeared in legs, wings, thorax, and abdomen of this insect. When cultured human keratinocytes were exposed to UVB radiation there was a significant increase in the expression of 2 clock genes, alpha- period 1 and alpha-clock that are believed to play an important role in controlling cellular circadian activity (Figure 3) (40).
Sunlight, UV Radiation and Heart Health
Season has a dramatic influence on cardiac mortality (41,42). It has been reported that cardiac mortality significantly increases by 22% and 31% in Norwegian and Irish men and by 24% and 39% in Norwegian and Irish women in the winter compared to the summer (43). This observation supports reports that serum cholesterol levels and blood pressure are lower during the summer compared to winter in both men and women (44, 45). It was also observed that both systolic and diastolic blood pressure increases as distances from the equator increases (46). A 6-week study of 18 patients with chronic kidney disease aged 26-66 years who were exposed to either UVB or UVA radiation reported that those exposed to UVA radiation had no change in their blood pressure, whereas those exposed to UVB radiation had a statistically significant decrease in both their systolic and diastolic blood pressures (47). At baseline both patient groups were found to be vitamin
D-deficient. The group receiving UVA radiation demonstrated no change in their circulating level of 25(OH)D, whereas the group receiving UVB radiation increased their blood level by 180% into the sufficient range (47). A follow-up study found that 26 weeks of exposure to UVB radiation was able to maintain a normal blood pressure in hypertensive patients for the duration of the 26-week study. After the UVB irradiation was halted the patients’ blood pressure was monitored for an additional 9 months and the patients remained normotensive.
The mechanism(s) involved in the observation that hypertension and cardiovascular disease correlate with latitude and rise in the winter is not well understood. Part of the explanation could be due to the increased production of vitamin D3. Several reports have suggested that vitamin D deficiency is associated with hypertension cardiovascular disease and cardiovascular mortality (48-54). A study in teenagers who received 2,000 IUs vitamin D3 daily for 4 months had a significant reduction in vascular stiffness (55).
Figure 4. Schematic representation of the synthesis and metabolism of vitamin D for skeletal and non-skeletal function. During exposure to sunlight, 7-dehydrocholesterol in the skin is converted to previtamin D3. Previtamin D3 immediately converts by a heat-dependent process to vitamin D3. Excessive exposure to sunlight degrades previtamin D3 and vitamin D3 into inactive photoproducts. Vitamin D2 and vitamin D3from dietary sources are incorporated into chylomicrons, transported by the lymphatic system into the venous circulation. Vitamin D (D represents D2 or D3) made in the skin or ingested in the diet can be stored in and then released from fat cells. Vitamin D in the circulation is bound to the vitamin D-binding protein (DBP), which transports it to the liver, where vitamin D is converted by the vitamin D-25-hydroxylase to 25- hydroxyvitamin D [25(OH)D]. This is the major circulating form of vitamin D that is used by clinicians to measure vitamin D status (although most reference laboratories report the normal range to be 20100 ng/ml, the preferred healthful range is 30-60 ng/ml). It is biologically inactive and must be converted in the kidneys by the 25-hydroxyvitamin D-1a-hydroxylase (1-OHase) to its biologically active form 1,25- dihydroxyvitamin D [1,25(OH)2D]. 1,25(OH)2D3 is then taken up by target cells and targeted to intracellular D-binding proteins (IDBP) to mitochondrial 24-hydroxylase or to the vitamin D receptor (VDR). The 1,25(OH)2D3-VDR complex heterodimerizes with the retinoic acid receptor (RXR) and binds to specific sequences in the promoter regions of the target gene. The DNA bound heterodimer attracts components of the RNA polymerase II complex and nuclear transcription regulators. Serum phosphorus, calcium fibroblast growth factors (FGF-23), and other factors can either increase or decrease the renal production of 1,25(OH)2D. 1,25(OH)2D feedback regulates its own synthesis and decreases the synthesis and secretion of parathyroid hormone (PTH) in the parathyroid glands. 1,25(OH)2D increases the expression of the 25- hydroxyvitamin D-24-hydroxylase (24-OHase) to catabolize 1,25(OH)2D to the water-soluble, biologically inactive calcitroic acid, which is excreted in the bile. 1,25(OH)2D enhances intestinal calcium absorption in the small intestine by stimulating the expression of the epithelial calcium channel (ECaC) and the calbindin 9K (calcium-binding protein, CaBP). 1,25(OH)2D is recognized by its receptor in osteoblasts, causing an increase in the expression of the receptor activator of the NF-kB ligand (RANKL). Its receptor RANK on the preosteoclast binds RANKL, which induces the preosteoclast to become a mature osteoclast. The mature osteoclast removes calcium and phosphorus from the bone to maintain blood calcium and phosphorus levels. Adequate calcium and phosphorus levels promote the mineralization of the skeleton. Autocrine metabolism of 25(OH)D; when a macrophage or monocyte is stimulated through its toll-like receptor 2/1 (TLR2/1) by an infectious agent such as Mycobacterium tuberculosis or its lipopolysaccharide, the signal up- regulates the expression of VDR and 1-OHase. A 25(OH)D level of 30 ng/ml or higher provides adequate substrate for 1-OHase to convert 25(OH)D to 1,25(OH)2D in mitochondria. 1,25(OH)2D travels to the nucleus, where it increases the expression of cathelicidin, a peptide capable of promoting innate immunity and inducing the destruction of infectious agents such as M. tuberculosis. It is also likely that the 1,25(OH)2D produced in monocytes or macrophages is released to act locally on activated T lymphocytes, which regulate cytokine synthesis, and activatedB lymphocytes, which regulate immunoglobulin synthesis. When the 25(OH)D level is approximately 30 ng/ml, the risk of many common cancers is reduced. It is believed that the local production of 1,25(OH)2D in the breast, colon, prostate, and other tissues regulates a variety of genes that control proliferation, including p21 and p27, as well as genes that inhibit angiogenesis and induce differentiation and apoptosis. Once 1,25(OH)2D completes the task of maintaining normal cellular proliferation and differentiation, it induces expression of the enzyme 24- OHase, which enhances the catabolism of 1,25(OH)2D to the biologically inert calcitroic acid. Thus, locally produced (autocrine) 1,25(OH)2D does not enter the circulation and has no influence on calcium metabolism. The parathyroid glands have 1-OHase activity, and the local production of 1,25(OH)2D inhibits the expression and synthesis of parathyroid hormone. The 1,25(OH)2D produced in the kidney enters the circulation and can down-regulate rennin production in the kidney and stimulate insulin secretion in the beta islet cells of the pancreas. (With permission Holick copyright 2013).
It is also known that the skin has the ability to produce nitric oxide (NO) a known vasodilator (41). When 24 healthy volunteers were exposed to 2 standard erythemal doses of UVA radiation their blood pressure substantially decreased. Further studies revealed that UVA radiation of the forearm increased blood flow independent of NO synthase (NOs) activity. It was observed that the UVA irradiation enhanced the release of cutaneous NO stores (56).
There are other factors that may also play a role in explaining why less sun exposure is associated with hypertension, cardiovascular disease and cardiovascular mortality. Exposure to UVB radiation causes the release of carbon monoxide from hemoglobin. carbon monoxide can cause vasodilation (57). There is also evidence that during sun exposure that substance P and calcitonin gene-related peptide are also produced in the skin. Both of these are known vasodilators (Figure 3) (58).
Sunlight, Autoimmune and Infectious Diseases
similar to cardiovascular disease it has been reported that there is an inverse association with increased risk for developing multiple sclerosis and type 1 diabetes and latitude (59-61). A person living at the equator has a 10-15 fold lower risk of developing type 1 diabetes (62). A person born and living at a latitude below 35° North had a 50% lower risk of developing multiple sclerosis later in life (59). It has also been reported that women who had the highest intake of vitamin D, had a reduced risk of developing multiple sclerosis by 41% (63) and rheumatoid arthritis by 44% (17). In a mouse model, naturally prone to developing type 1 diabetes, treatment with 1,25(OH D3 throughout their life reduced their risk of developing type 1 diabetes by more than 90% (64). A study in Finland revealed that infants during the first year of life in the 1960s who had received 2,000 IU of vitamin D3 daily for the first year of life reduced their risk of developing type 1 diabetes later in life by 88% (65).
In a mouse model for multiple sclerosis it was found that exposure to UVB radiation was more effective than 1,25(OH)2D3 in reducing signs of experimental autoimmune encephalitis (66).
Although there is strong evidence to support that improvement in vitamin D status in early life may decreased risk for many autoimmune diseases, there are likely additional benefits from exposure to ultraviolet radiation. One potential benefit may be due to the increased expression of the proopiomelanocortin (POMC) gene that not only results in the production of beta-endorphin, but also ACTH (adrenocorticotropin hormone) that increases the adrenal glands’ production of cortisol, a known modulator of the immune system (67).
Finsen received the Nobel Prize for the observation that exposure to sunlight was effective for treating a tuberculosis infection in the skin. It is now recognized that macrophages have a VDR and when they ingest an infectious agent, such as TB, toll-like receptors are activated. This activation results in the increased expression of the 1-alpha-hydroxylase. 25(OH)D that enters the macrophage is converted by this enzyme to 1,25(OH)2D. 1,25(OH)2D interacts with its VDR in the nucleus increasing the expression of the gene that produces cathelicidin. The increased production of cathelicidin, a defensen protein, results in the destruction of the infectious TB (68). It has also been observed that school children in Japan who received 1,200 IUs vitamin D3 daily during the winter reduced their risk of developing influenza A infection by more than 40% (69). It was also observed that these children had a 90% reduction in recurrent asthmatic attacks. Healthy adults who maintained on average a blood level of 25(OH)D of 38 ng/mL reduced their risk of developing acute viral respiratory tract infections two-fold (17).
Application of Visible and Near Infrared Radiation for Skin Health
The efficacy of red, blue and near-infrared light treatments have been evaluated for wound healing, reduction in fine lines, wrinkles and improving dermal collagen density (Figure 1). In one study ultrasonography of skin samples before and after 30 treatments of red light and energizing light technology revealed substantial improvements in the dermal collagen matrix with increased thickness. Follow-up clinical photography revealed improvement changes in wrinkles and skin roughness (70).
Sunlight and Cancer
In 1915 it was reported that indoor workers had an 8-times higher risk of dying of cancer compared to outdoor workers (71). In 1941 Apperly reported that people living in the Northeast had a much higher risk of dying of cancer compared to people living in the southern states of the United States (72). In the 1980s Garland et al. reported that there was a higher risk of developing colorectal cancer for those who lived at a higher latitude in the United States (73). This followed with the report that there was an association with risk for developing colorectal cancer and vitamin D deficiency (74). It was suggested that 1,000 IUs vitamin D daily reduced the risk of colorectal cancer by as much as 50%. These seminal observations were followed by a multitude of ecological and association studies relating vitamin D deficiency and living at higher latitudes with increased risk for developing a variety of cancers and increased cancer mortality (75-83).
A study of women in Canada revealed that women who had the most sun exposure between the ages of 10-19 years of age had a 69% reduced risk of developing breast cancer later in life compared to women who had the least sun exposure during the same period of time (84).
Although the exact mechanisms by which sunlight helps reduce risk for developing many deadly cancers is not known, what is known is that many cells in the body can locally convert 25(OH)D to 1,25(OH D (28, 30-32). By doing so the 1,25(OH D interacts with its receptor in the cell to unlock a wide variety of genes. It is been estimated that upwards of 2,000 genes may be directly or indirectly regulated by 1,25(OH D (31, 32, 85). In a study of healthy adults who received 2,000 IUs of vitamin D3 daily for 12 weeks found that compared to baseline 291 genes in their white cells were significantly altered. These genes were related to more than 80 different pathways that control among other biologic processes DNA repair, apoptosis, oxidative stress and anti-inflammatory activity all of which can be associated with malignancy (Figure 5) (31).
Conclusion
It is an undisputable fact that living at higher latitudes and having less sun exposure increases risk for many chronic illnesses, infectious diseases and mortality. Even birth month affects lifetime disease risk (86). A recent study reported widespread seasonal gene expression demonstrating marked annual differences in genes affecting immunity and physiology (87). Female mice exposed to ultraviolet B radiation resulted in a signaling system in the arcuate nucleus resulting in the expression of the POMC gene. This resulted in an increase in the blood levels of beta endorphin and alpha-MSH (88). This observation suggests that exposure to ultraviolet B radiation on the skin also has a profound far- reaching influence on brain activity.
Another undisputable fact is that the major source of vitamin D for most humans is sun exposure. A study in Maasai herdsman who lived near the equator and are outside exposed to sunlight on a daily basis were found to have a blood level on average of 25(OH)D of 48 ng/mL (89). Thus it is likely that our hunter-gather forefathers exposed to sunlight on a daily basis were maintaining blood levels in the same range; a range similar to what was suggested by the Endocrine Practice Guidelines i.e. a 25(OH)D of 40-60 ng/mL for maximum bone health and overall health and wellbeing. There is no downside to improving vitamin D status with the exception of some patients with granulomatous disorders who have a hypersensitivity to vitamin D (90). To achieve a healthy lifestyle, sensible sun exposure, exercise and maintenance of a serum 25(OH)D of at least 30 ng/ml (preferably 40-60 ng/ml) is required. The European code against cancer 4th edition acknowledges that the beneficial effects of sun for producing vitamin D can be fully achieved while still voiding too much sun exposure (91). To maintain a serum 25(OH)D in a healthy range three approaches are suggested. ingesting foods that naturally contain or are fortified with vitamin D can help provide some of the vitamin D requirement. Sensible sun exposure during the spring and summer and fall will improve vitamin D status. Because so many factors influence sun induced vitamin D3 synthesis an app, dminder.info, was developed to provide guidance for sensible sun exposure and reducing risk for sun burning. To guarantee vitamin D sufficiency a vitamin D supplement should also be used on a daily basis. For children 1,000 IUs and for adults 2,000 IUs daily will maintain blood levels of 25(OH)D above 30 ng/mL. For those who are obese they may require at least 2-3 times more to satisfy their requirement.
References
Holick MF: Vitamin D: A millennium perspective. J Cell Biochem 88: 296-307, 2003.
Holick MF, Tian XQ and Allen M: Evolutionary importance for the membrane enhancement of the production of vitamin D3 in the skin of poikilothermic animals. Proc Natl Acad Sci USA 92: 3124-3126, 1995.
Halliday GM and Byrne SN: An unexpected role: UVA induced release of nitric oxide fomr skin may have unexpected health benefits. J Int Derm 134: 1791-1794, 2014.
Pathak M A et al: Photobiology of melanin pigmentation: dose/response of skin to sunlight and its contents. J Am Acad Dermatol 9: 724-733, 1983.
Setlow RB: Cyclobutane-Type pyrimidine dimers in polynucleotides. Science 153(3734): 370-386, 1966.
Duncan B and Miller J: Mutagenic deamination of cytosine residues in DNA. Nature 287: 560-561, 1980.
Whitemore SE, Potten CS, Chadwick, A, Strickland PT and Morison WL: Effect of photoreactivating light on UV-radiation- induced alterations in human skin. Photodermatol Photoimmunol Photomed 17(5): 213-217, 2001.
Essen LO and Klar T: Light Drive DNA repair by photolysases. Cell Mol Life Sci 63(11): 1266-1277, 2006.
Friedberg E: DNA Damage and Repair. Nature 421: 436-439, 2003.
Arie VA and Len R: Biological consequences of cyclobutane pyrimidine dimers. Journal of Photochemistry and Photobiology B:Biology 65(2-3): 101-104, 2001.
Brash DE et al: A role for sunlight in skin cancer: UV-induced p53 mutations in squamous cell carcinoma. Proc Natl Acad Sci 88: 10124-128, 1991.
Kennedy C, Bajdik CD, Willemze R, De Gruijl FR, Bouwes and Bavinck JN: The influence of painful sunburns and lifetime sun exposure on the risk of actinic keratoses, seborrheic warts, melanocytic nevi, atypical nevi, and skin cancer. J Invest Dermatol 120: 1087-1093, 2003.
Wang SQ, Balagula Y and Osterwalder U: Photoprotection: a review of the current and future technologies. Dermatol Ther 23: 31-47, 2010.
Sjerobabski MI and Poduje S: Photoaging. Coll Antropol 32(Suppl 2): 177-180, 2008.
Vink AA, Yarosh DB and Kripke ML: Chromophore for UV- induced immunosuppression: DNA. Photochem Photobiol 63: 383-386, 1996.
Holick MF: Biologic effects of light: historical and new perspectives. In: ME. Holick and E.G. Jung (eds.) Biologic Effects of Light. Boston: Kluwer Academic Publishers 11-32, 1999.
Wacker M and Holick MF: Sunlight and Vitamin D: A global perspective for health. Dermato-Endocrinol 5(1): 51-108, 2013.
Molozolowski W and Sniadecki J: (1786-1883) on the cure of rickets. Nature 143: 121, 1939.
Palm TA: The geographic distribution and etiology of rickets. Practitioner 45: 270-279, 321-342, 1890.
Rajakumar K, Greenspan SL, Thomas SB and Holick MF: SOLAR ultraviolet radiation and vitamin D: a historical perspective. Am J Public Health 97: 1746-1754, 2007.
Huldschinsky K: Heilung von Rachitis durch Kunstliche Hohensonne. Deutsche Medizinische Wochenschrift 90-91, 1919.
Hess AF and Unger LJ: Use of the carbon arc light in the prevention and cure of rickets. JAMA 78(21): 1596-1598, 1922.
Steenbock H and Black A: The reduction of growth-promoting and calcifying properties in a ration by exposure to ultraviolet light. J Biol Chem 61: 408-422, 1924.
Wolf G: The Discovery of Vitamin D: The Contribution of Adolf Windaus. J Nutr 134: 1299-1302, 2004.
Lightwood R, Sheldon W and Harris C: Hypercalcaemia in infants and vitamin D. BMJ 2: 149, 1956.
Holick MF: Vitamin D Is Not as Toxic as Was Once Thought: A Historical and an Up-to-Date Perspective. Mayo Clinic Proc 90(5): 561-564, 2015.
Pober BR: Williams Beuren Syndorme. N Eng J Med 362(3): 239-252, 2010.
Holick MF: Vitamin D deficiency. New Engl J Med 357: 266268,2007.
Hossein-nezhad A and Holick MF: Vitamin D for Health: A Global Perspective. Mayo Clin Proc 88(7): 720-755, 2013.
Adams JS and Hewison M: Update in Vitamin D. J Clin Endocrinol Metab 95(2): 471-478, 2010.
Hossein-nezhad A, Spira A and Holick MF: Influence of Vitamin D Status and Vitamin D3 Supplementation on Genome Wide Expression of White Blood Cells: A Randomized Double-Blind Clinical Trial. PLoS ONE 8(3): e58725, 2013.
Montecino M, Stein GS, Stein JL, Lian JB, Wijnen AJ, Carvallo L, Marcellini S, Cruzat F and Arriagada G: Vitamin D control of gene expression: Temporal and spatial parameters for organization of the regulatory machinery. Crit Rev Eukaryot Gene Expr 18(2): 163-172, 2008.
Zanello S, Jackson D and Holick MF: An immunocytochemical approach to the study of beta-endorphin production in human keratinocytes using confocal microscopy. Ann NY Acad Sci 885: 85-99, 1999.
Jussila A, Huotari-Orava R, Ylianttila L, Partonen T and Snellman E: Narrowband ultraviolet radiation induces the expression of -endorphin in human skin in vivo. J Photochem Photobiol B 155: 104-108, 2016.
Fell GL, Robinson KC, Mao J, Woolf CJ and Fisher DE: Skin |3-Endorphin mediates addiction to UV light. Cell 157: 15271534, 2014.
Lewy A, Rough J, Songer J, Mishra N, Yuhas K and Emens J: The phase shift hypothesis for the circadian component of winter depression. Dialogues in Clinical Neuroscience 9: 3, 2007.
Rosenthal NE, Sack DA, Gillin JC, Lewy AJ, Goodwin FK, Davenport Y, Mueller PS, Newsome DA and Wehr TA: Seasonal affective disorder: a description of the syndrome and preliminary findings with light therapy. Arch Gen Psychiatry 41: 72-80, 1984.
Lewy AJ, Sack RL and Singer CMN: Assessment and treatment of chronobiologic gate model and the phase response curve. Psychopharmacol Bull 20: 561-565, 1984.
Pennisi E: Multiple clocks keep time in fruit fly tissues. Science 278(5343): 1560-1561, 1997.
Zanello SB, Jackson D and Holick MF: Expression of the circadian clock genes clock and period 1 in human skin. J Invest Dermatol 115(4): 757-760, 2000.
Juzeniene A, Brekke P, Dahlback A, Andersson-Engels S, Reichrath J, Moan K, Holick MF, Grant WB and Moan J: Solar Radiation and Human Health. Rep Prog Phys 74: 1-56, 2011.
Scragg R: Seasonality of cardiovascular disease mortality and the possible protective effect of ultra-violet radiation. Int J Epidemiol 10: 337-344, 1981.
Eng H and Mercer JB: Seasonal Variations in Mortality Caused by Cardiovascular Diseases in Norway and Ireland. Journal of Cardiovascular Risk 5: 89-95, 1998.
Ockene IS, Chiriboga DE, Stanek EJ 3rd, Harmatz MG, Nicolosi R, Saperia G, Well AD, Freedson P, Merriam PA, Reed G, Ma Y, Matthews CE, Hebert JR: Seasonal variation in serum cholesterol levels: treatment implications and possible mechanisms. Arch Intern Med 26;164(8): 863-870, 2004.
Charach G, Rabinovich PD and Weintraub M: Seasonal changes in blood pressure and frequency of related complications in elderly Israeli patients with essential hypertension. Gerontology 50(5): 315-321,2004.
Rostand SG: Ultraviolet light may contribute to geographic and racial blood pressure differences. Hypertension 30: 150-156, 1997.
Krause R, Buhring M, Hopfenmuller W, Holick MF and Sharma AM: Ultraviolet B and blood pressure. Lancet 352: 709-710, 1998.
Giovannucci E, Liu Y, Hollis BW and Rimm EB: 25- hydroxyvitamin D and risk of myocardial infarction in men: a prospective study. Arch Intern Med 168: 1174-1180, 2008.
Dobnig H, Pilz S, Scharnagl H, Renner W, Seelhorst U, Wellnitz B, Kinkeldei J,Boehm BO, Weihrauch G and Maerz W: Independent association of low serum 25-hydroxyvitamin D and 1,25-dihydroxy vitamin D levels with all-cause and cardiovascular mortality. Arch Intern Med 168: 1340-1349, 2008.
Pilz S, Dobnig H, Fischer JE, Wellnitz B, Seelhorst U, Boehm BO and Marz W: Low vitamin D levels predict stroke in patients referred to coronary angiography Stroke 39: 26112613,2008.
Ginde AA, Scragg R, Schwartz RS and Camargo CA Jr.: Prospective study of serum 25-hydroxyvitamin D level, cardiovascular disease mortality, and all-cause mortality in older US adults. J Am Geriatr Soc 57: 1595-1603, 2009.
Kilkkinen A, Knekt P, Aro A, Rissanen H, Marniemi J, Heliovaara M, Impivaara O and Reunanen A: Vitamin D status and the risk of cardiovascular disease death Am J Epidemiol 170: 1032-1039, 2009.
de Boer IH, Kestenbaum B, Shoben AB, Michos ED, Sarnak MJ and Siscovick DS: 25-hydroxyvitamin D levels inversely associate with risk for developing coronary artery calcification. J Am Soc Nephrol 20: 1805-1812, 2009.
Wang L, Manson JE, Song Y and Sesso HD: Systematic Review: Vitamin D and calcium supplementation in prevention of cardiovascular events. Ann Intern Med 152: 315-323, 2010.
Dong Y, Pollock N, Stallmann-Jorgenssen IS, Gutin B, Lan L, Chen TC, Keeton D, Petty K, Holick MF and Zhu H: Low 25- Hydroxyvitamin D Levels in Adolescents: Race, Season, Adiposity, Physical Activity, and Fitness. Pediatr 125(6): 1104-1111,2010.
Liu D, Fernandez BO, Hamilton A, Lang NN, Gallagher JM, Newby DE, Feelisch M and Weller RB: UVA irradiation of human skin vasodilates arterial vasculature and lowers blood pressure independently of nitric oxide. Synthase. J Int Derm 143: 1839-1846, 2014.
Stec A, Heather D and Vera T: Role of Carbon Monoxide in Blood Pressure Regulation. Hypertension 51:597-604, 2008.
Mead MN: Benefits of Sunlight: A Bright spot for human health. Environ Health Perspect 116(4): A160-A167, 2008.
Kurtzke JF: Geographic distribution of multiple sclerosis: an update with special reference to Europe and the Mediterranean region. Acta Neurol Scand 62: 65-80, 1980.
van der Mei IA, Ponsonby AL, Dwyer T, Blizzard L, Simmons R, Taylor BV, Butzkueven H and Kilpatrick T: Past exposure to sun, skin phenotype, and risk of multiple sclerosis: case-control study. Br Med J 327: 316, 2003.
Wallin MT, Page WF and Kurtzke JF: Multiple sclerosis in US veterans of the Vietnam era and later military service: race, sex, and geography. Ann Neurol 55: 65-67, 2004.
Mohr SB, Garland CF, Gorham ED and Garland FC: The association between ultraviolet B irradiance, vitamin D status and incidence rates of type 1 diabetes in 51 regions worldwide. Diabetologia 51: 1391-1398, 2008.
Munger KL, Levin LI, Hollis BW, Howard NS and Ascherio A: Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis. JAMA 296: 2832-2838, 2006.
Mathiery C, Waer M, Casteels K, Laureys J and Bouillon R: Prevention of Type I Diabetes in NOD mice by nonhypercalcemic doses of a new structural analog of 1,25 dihydroxyvitamin D3, K 1060. Endocrinology 123: 866-872, 1995.
Hypponen E, Laara E, Reunanen A, Jarvelin MR and Virtanen SM: Intake of vitamin D and risk of type 1 diabetes: a birth- cohort study. Lancet 358: 1500-1503, 2001.
Becklund BR, Severson KS, Vang SV and DeLuca HF: UV radiation suppresses experimental autoimmune enecephalomye- litis independent of Vitamin D production. PNAS 107(14): 64186423,2010.
Slominski A: A nervous breakdown in the skin: stress and the epidermal barrier. J Clin Invest 117(11): 3166-3169, 2007.
Liu PT, Stenger S, Li H, Wenzel L, Tan BH, Krutzik SR, Ochoa MT, Schauber J, Wu K, Meinken C, Kamen DL, Wagner M, Bals R, Steinmeyer A, Zugel U, Gallo RL, Eisenberg D, Hewison M, Hollis BW, Adams JS, Bloom BR and Modlin RL: Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 311: 1770-1773,2006.
Urashima M, Segawa T, Okazaki M, Kurihara M, Wada Y, Ida H: Randomized trial of vitamin D supplementation to prevent seasonal influenza A in school children. Am J Clin Nutr 91: 1255-1260, 2010.
Wunsch A and Matuschka K: A controlled trial to determine the efficacy of red and nearinfrared light treatment in patient satisfaction, reduction of fine lines, wrinkles, skin roughness, and intradermal collagen density increase. Photomed Laser Surg 32(2): 93-100, 2014.
Hoffman F: The Mortality of Cancer throughout the World. Appendix E, Prudential Press, 1915.
Apperly FL: The Relation of Solar Radiation to Cancer Mortality in North America. Cancer Res 1: 191-5, 1941.
Garland CF and Garland FC: Do sunlight and vitamin D reduce the likelihood of colon cancer? Int J Epidemiol 9: 227-231, 1980.
Garland C, Shekelle RB, Barrett-Connor E, Criqui MH, Rossof AH and Paul O: Dietary vitamin D and calcium and risk of colorectal cancer: a 19-year prospective study in men. Lancet 1: 307-309, 1985.
Garland CF, Comstock GW, Garland FC, Helsing KJ, Shaw EK and Gorham ED: Serum 25-hydroxyvitamin D and colon cancer: eight-year prospective study. Lancet 334: 1176-1178, 1989.
Garland FC, Garland CF, Gorham ED, Miller MR, Brodine SK, Fallon A and Balazs LL: Geographic variation in breast cancer mortality in the United States: a hypothesis involving exposure to solar radiation. Prev Med 19: 614-622, 1990.
Lefkowitz ES and Garland CF: Sunlight, vitamin D, and ovarian cancer mortality rates in US women. Int J Epidemiol 23: 11331136, 1994.
Grant WB: An estimate of premature cancer mortality in the US due to inadequate doses of solar ultraviolet-B radiation. Cancer 94: 1867-1875, 2002.
Garland CF, Mohr SB, Gorham ED, Grant WB and Garland FC: Role of ultraviolet B irradiance and vitamin D in prevention of ovarian cancer. Am J Prev Med 31: 512-514, 2006.
Mohr SB, Garland CF, Gorham ED, Grant WB and Garland FC: Relationship between low ultraviolet B irradiance and higher breast cancer risk in 107 countries. Breast J 14: 255-260, 2008.
Grant WB and Mohr SB: Ecological studies of ultraviolet B, vitamin D and cancer since 2000. Ann Epidemiol 19: 446-454, 2009.
Giovannucci E, Liu Y, Rimm EB, Hollis BW, Fuchs CS, Stampfer MJ and Willett WC: Prospective study of predictors of vitamin D status and cancer incidence and mortality in men. J Natl Cancer Inst 98: 451-459, 2006.
Grant WB: Relation between prediagnostic serum 25- hydroxyvitamin D level and incidence of breast, colorectal, and other cancers. J Photochem Photobiol B 101: 130-136, 2010.
Knight JA, Lesosky M, Barnett H, Raboud JM and Vieth R: Vitamin D and reduced risk of breast cancer: a population-based case-control study. Cancer Epidemiol Biomarkers Prev 16: 422429,2007.
Tarroni P, Villa I, Mrak E, Zolezzi F, Mattioli M, Gattuso C and Rubinacci A: Microarray analysis of 1,25(OH^D3 regulated gene expression in human primary osteoblasts. J Cell Biochem 113(2): 640-649, 2012.
Boland MR, Shahn Z, Madigan D, Hripcsak G and Tatonetti NP: Birth month affects lifetime disease risk: A phenome-wide method. J Am Med Inform Assoc 0: 1-15, 2015.
Dopico XC, Evangelou M, Ferreira RC, Guo H, Pekalski ML, Smyth DJ, Cooper N, Burren OS, Fulford AJ, Hennig BJ, Prentice AM, Ziegler AG, Bonifacio E, Wallace C and Todd JA: Widespread seasonal gene expression reveals annual differences in human immunity and physiology. Nature comm 6: 1-13, 2015.
Skobowait C and Slominski AT: Ultraviolet B stimulates proopiomelanocortin signaling in the arcuate nucleus of the hypothalamus in mice. Exp Dermatol 25: 20-123, 2016.
Luxwolda MF, Kuipers RS, Kema IP, Dijck-Brouwer DA and Muskiet FAJ: Traditionally living populations in East Africa have a mean serum 25-hydroxyvitamin D concentration of 115 nmol/l. Br J Nutr 108: 1557-1561,2012.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Murad MH and Weaver CM: Evaluation, Treatment & Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 96(7): 1911-1930, 2011.
Greinert R, de Vries E, Erdmann F, Espina C, Auvinen A, Kesminiene A and Schuz J: European code cancer fourth edition: Ultraviolet radiation and cancer. Cancer Epidemiol 39: S75-83, 2015.