Original in Portuguese
A few of the many Coimbra articles on Vitamin D Life
- Interview of Dr. Coimbra: MS, Autoimmune, Vitamin D, B2, Ca, Mg, PTH etc. – perhaps 2018
- Vitamin D has treated Multiple Sclerosis and autoimmune diseases for 16 years – Coimbra April 2018
- Dr. Coimbra interview covering Vitamin D, Magnesium, Folate, Vaccines - Oct 2018
- Multiple Sclerosis Coimbra Protocol stories on Facebook
- Dr. Coimbra discusses Vitamin D, Magnesium, Folic Acid, B12, Autism, Depression, etc – Sept 2018
- Guide for patients on high doses of Vitamin D – Coimbra 2017
- High-Dose Vitamin D Therapy – book July 2018
- Most of Coimbra Protocol supplements in a capsule taken 4 times a day – June 2019
The following is from a Google Translation
The fallacy of the absence of evidence from the Coimbra Protocol
Over the last almost four years I have been privileged to be part of a team of more than 120 physicians worldwide who use vitamin D every day to try and reverse autoimmune diseases such as multiple sclerosis, lupus or rheumatoid arthritis. Although relatively extensive in Europe, my experience is manifestly small when we consider that the Coimbra Protocol has 18 years of development , fruit of the dedicated and continuous work of the brilliant Professor Cícero Coimbra. Globally, there are probably more than 20,000 people being treated with vitamin D, achieving varying degrees of success and, because they also exist, failure. Fortunately, the former are incredibly more frequent than the latter , making daily reports of improvements in supposedly non-breeding diseases.It is not a conventional or conventionally prescribed treatment , making it very susceptible to criticism, skepticism and, in general, attacks. Some criticisms or attacks are reasonable: to say "taking high-dose vitamin D is a highly dangerous and potentially catastrophic practice" is probably a euphemism. It is 100% true that, under certain very specific conditions, the Coimbra Protocol can create a state of hypercalcaemia - excess of calcium in the blood. From the moment this state is created, a thousand and problems arise. From renal calcification to cardiovascular and endocrine disorders. It is, in fact, a fair criticism. But there is a "but . " And it's a big "but":this state of hypercalcaemia is totally preventable and its development depends literally on the will of the person to create it . It can be totally avoidable , following the specific indications of food alteration and water reinforcement necessary However, the main attack on the Coimbra Protocol is not this possible damage that may cause but " lack of clinical evidence for the use of vitamin D in the treatment of autoimmune diseases ." It is the argument most often used to dissuade anyone who thinks about fighting for their health and fighting their disease in another way.Sorry to say but the argument is false! The evidence exists, is vast and justifies its use.
The science of the Coimbra Protocol
Let us begin by addressing the question of what the Coimbra Protocol does not have , trying to eliminate the most commonly used argument at the outset: there is no published study to support treatment with high doses of vitamin D in autoimmune diseases. It is not true: it exists . In 2014 an article was published in the journal DermatoEndocrinology on the effect of 35000UI of vitamin D daily during 6 months in patients with vitiligo and psoriasis . The results are very close to fantastic: more than 85% of the people with vitiligo had between 25 and 75% of the lesions with evidence of repigmentation and 100% of those with psoriasis had significant clinical improvement of the cutaneous lesions. However, the study has obvious technical limitations: it is not a randomized clinical trial (RCT), it is an extremely small study regarding the number of participants and the pathologies studied can be considered as "minor" (although not there is nothing minor in the emotional suffering caused by the social stigma associated with the cutaneous alterations of these pathologies). Therefore, and following the medical rationale of "only therapeutic attitudes that have RCTs to demonstrate their efficacy should be used in current medical practice", the Coimbra Protocol could not be considered as scientifically supported.However, the "counter-argument" is brought to us by some of the most respected and reputed medical journals and is broken down into several parts .Let us begin here: in 2003 an article was published in the British Medical Journal , with this conclusion:
- Hormones
- With pleiotropic effects
- There is no ideal dosage for all, needing to adjust case by case and control analytically over time
- Its sub-dosage has no clinical effect
- Over-dosage includes serious, potentially catastrophic, health hazards.
Given that vitamin D is also a hormone with pleiotropic effect and the dosage should be adjusted case by case, at risk of not being effective or being highly dangerous, not accepting its use while accepting the use of levothyroxine or insulin is have different weights for very similar therapeutic approaches !Before we focus on the science that supports and justifies vitamin D and its use in autoimmune diseases, a very small introduction is important to the pathophysiological processes underlying these pathologies.
The autoimmunity equation
The basic equation of autoimmunity can be considered as:AI = Treg - Th17This means that the development of autoimmune diseases (AI) occurs when there is an imbalance between regulatory T cells (Treg, immune cells whose role is to control the function of immune cell lines) and helper T cells 17 (Th17, immune cells which, for besides the role they have in defending the body against some bacteria, are the cellular basis of the development of various autoimmune diseases). While the action of Treg cells is able to overlap and control the intensity of Th17 function, the development of auto-attack mechanisms will have a great deal of difficulty. In therapeutic terms,the recovery of this balance is the ultimate goal, it is the Holy Grail: this would mean blocking the reason for the existence of autoimmune diseases!This is the first point in favor of the use of vitamin D in these pathologies: during the last years, the attention aroused by the role of vitamin D immunity has led to the publication of hundreds of articles in the most varied international magazines . In this study published in the journal Clinical Reviews of Allergy and Immunology it is concluded by the authors that"Due to its unique ability to bind to VDR and serves as a transcriptional factor, vitamin D can regulate gene expression and further exert its immuno-modulatory effects on immune cells. It has been shown to inhibit Th17 cytokine production, enhance Treg activity, induce NKT cell functions, suppress Th1, and promote Th2 cytokine production, and thus skew T cells toward Th2 polarization "In this other , published in the Journal of Neuroimmunology , it is said that"(...) the results indicate that the active form of vitamin D added to polyclonally-activated T cells from MS patients is able to reduce the proportion of pathogenic T cells, defined by the ability to produce IL-17 with or without IFN-γ cytokines "They are not unique cases. The existing evidence seems to indicate that when there is a low effect or low concentration of vitamin D, there is a trend towards the further development of these pro-attacking cell lines, to the detriment of Treg regulatory cells , creating the pathophysiological conditions for the onset of diseases autoimmune diseases. On the other hand, the above conclusions are quite clear and evident: the increase in the biological effect of vitamin D is able to inhibit the production of Th17 cells and increase Treg cells! I repeat, because it deserves it: the biological effect of vitamin D can achieve the ideal goal of treatments for autoimmune diseases: more Treg and less Th17!Therefore, more Vitamin D seems to mean less Autoimmunity!A myriad of observational studies have been published over the past few years showing a relationship between decreased levels of vitamin D and increased incidence or aggressiveness of various autoimmune diseases such as multiple sclerosis , systemic lupus erythematosus , rheumatoid arthritis , Crohn's disease , Hashimoto's thyroiditis , vitiligo or psoriasis .The relationship between low levels of vitamin D and the development of autoimmune diseases seems to be less and less questionable . However, as advocated in evidence-based medicine - well, correlation does not mean causality.
How much vitamin D is needed?
Given the existing evidence, the question to be asked is " what concentration of vitamin D is required for the body to achieve this biological goal and optimize its function? ".It is true that the body is able to produce vitamin D - but exposing the skin to the sun over an extended period of time, without sunscreen, at a time when the incidence of UVB rays is sufficient for the process of transforming 7-dehydrocholesterol into cholecalciferol to happen and trigger the production cascade of the active form of vitamin D. It is estimated that this period is approximately 20 to 30 minutes in the summer. Unfortunately, the Western lifestyle makes it impossible to expose ourselves to the sun for half an hour throughout the year , justifying the lowlevels of vitamin D in the world . While it is true that in theory the body could produce enough vitamin D,in fact, this self-production has no practical clinical relevance because, even in countries that live on the beach like Brazil, the prevalence of vitamin D deficiency is quite high. It is then necessary to supplement so that adequate blood levels of this vital hormone can be achieved .Current recommendations for vitamin D supplementation with 600 to 800 IU daily were considered statistically wrong in 2014 , an argument published in an article published in the journal Nutrients , and the daily dose is considered adequate to achieve normal blood levels of 8895 IU cholecalciferol .This means that supplementation with these "high" doses should be enough to control autoimmune diseases and achieve the desired immune balance, right? Unfortunately, not always . There are several articles to show that even taking doses higher than the recommended "normal" 800 IU daily does not seem to affect the symptoms of multiple sclerosis ( this or this ). Otherwise, we can say that ideal levels of vitamin D in the blood do not appear to have a real clinical impact on autoimmune diseases . There are, however, some publications in which these same doses have been shown to be effective and clinically meaningful. In this studypublished in the journal Immunology Research , nor were doses higher than those defined as safe by the European Food Safety Authority to achieve very significant results at analytical or even clinical level !!!How then is this dissociation between the effects demonstrated by vitamin D in the balance Treg vs Th17 and the absence of positive clinical effect in these studies? To do this, allow a small deviation.
The history of the Perfect Factory and the Real Factory
Imagine visiting the best tableware factory in the country, with a high level of quality and profitability. Let's call it Perfect Factory . He is so impressed that he wants to replicate this same factory, aiming to achieve the same level of success. To do this, study hard and find that it produces 100 tables per day, using for that 1000 kg of wood that are worked by an incredibly calibrated and optimized assembly line. It is able to unveil what kind of machinery is the line and how it works, and is then prepared to set up your factory. Let's call it Real Factory . Although exactly the same wood can be obtained , it is no longer possible to obtain exactly the same assembly line. However, the supplier tells you that you have another model, slightly different, which is very similar and will do the same job. After having everything set up, your profit is compromised because the production capacity of the factory falls short of your expectations : although the same 1000 kg of wood enters the production unit, only 50 tables are produced per day.To save the Royal Factory , you have to find out where the problem lies and find a solution for it . It begins by pondering whether the problem will not be the quality of the wood, which may not allow to produce more tables. He abandons this hypothesis because it is the same wood that is used by the Perfect Factory. His attention is focused on the machines that make up the production line. Note that one of the main machines on your assembly line works in a slightly different way, with lower than expected profitability and is responsible for the smaller numbers .Having identified the problem, it is time to get a solution . After a few attempts, it concludes that by increasing the amount of wood at the beginning of the manufacturing process, it manages to mitigate the imperfection of the machine and increase the number of tables produced. Thus, it gradually raises the initial wood until it produces another 100 tables per day , making the Fábrica Real finally profitable.This metaphor explains the dissociation between laboratory studies , where it is demonstrated that vitamin D has the desired immunological effect, and the results of published clinical studies , which seem to indicate a lack of this clinical effect.As in the Perfect Factory, when the entire physiological process occurs optimally in the laboratory, vitamin D can have the intended effect of controlling the intensity of the Th17 response and increasing the Treg cells, decreasing the aggressiveness, intensity or even the prevalence of autoimmune diseases. However, in the Real Factory, given the malfunction of one of the machines, the real and practical effect of the same amount of raw material is less. Likewise, in "real life", taking the same form or quantity of vitamin D, effective in ideal situations, does not produce the same clinical results. This is demonstrated by the results published clinical studies. Although one can conclude that vitamin D has no clinical effect, this hypothesis should be excluded given the effect demonstrated in ideal situations. Following the metaphor of the Perfect Factory vs. Real Factory, we should try to find out if any, or what, "machine is malfunctioning," as our Royal Factory owner did.Several research teams thought the same way and tried to assess whether people with autoimmune diseases had a different machine whose action might be altered to the point of influencing the effective biological mechanism of vitamin D and thus influencing their clinical outcomes. For that, they looked at the programming we all have and the reading from which the various receptors, the various enzymes and the various proteins that are produced in our organism: the DNA .
Genetic variations of vitamin D and its relationship with autoimmune diseases
By researching among autoimmune patients the genetic peculiarities common to several "machines" that influence the biological metabolism of vitamin D, different teams of researchers were able to identify a higher frequency of single nucleotides polymorphisms ( SNP), small genetic variations, in the vitamin D receptor ( vitamin D receptor , VDR) in these patients . This has already been seen in several pathologies - multiple sclerosis , rheumatoid arthritis , Crohn's disease , Hashimoto's thyroiditis or lupus .This article on the genetic specificities of the vitamin D receptor associated with lupus deserves a more detailed evaluation for several reasons:
- It was written by a Portuguese research team , dedicated to the study of autoimmune diseases;
- It was performed in Portuguese patients ;
- Their conclusions are very clear and help to understand the clinical relevance of these small variations:
- Our study confirms a possible role of VDR gene polymorphisms in SLE .
- A positive association was found between VDR polymorphisms and SLE severity (chronic damage) .
- The presence of CT genotype of FokI and TT genotype of TaqI seems to confer a worse prognosis and may constitute a risk factor for higher long-term cumulative damage in SLE patient s .
According to the authors, the presence of these genetic characteristics seems to confer worse prognosis and be a risk factor for greater cumulative damage in patients with lupus! If we were talking about table plants, we would say that we could have found the machine defective, responsible for the difference between the perfect scenario and real life!To help support this hypothesis, it is necessary to understand whether biological differences resulting from the genetic variations identified have, however, a relevant clinical impact. There is already some published information on the subject. Each already identified genotype of the VDR confers a slight conformational change to its molecular structure, a slight three-dimensional difference, conditioning the binding of active vitamin D to the receptor . By not doing it perfectly, because there is no perfect fit, the action of the vitamin D receptor is compromised and the clinical effects of our hormone do not occur normally. In the same way that a less optimal wood-machine link caused the loss of profitability of the Real Factory, aimperfect functioning of the binomial Vitamin D receptor creates the conditions for an imperfect immune system .This may explain the dissociation between laboratory studies and published clinical studies: due to genetic alterations in patients with autoimmune diseases, taking normal doses or normally high doses (but less than 10,000 IU daily) of vitamin D is not enough to achieve a biological effect that alters the development of Th17 or Treg cells . Immune status does not change significantly with the currently recommended doses of vitamin D. However, concluding that these doses have no clinical effect can not lead one to conclude that vitamin D has no clinical effect on these diseases. Just as the owner of the Royal Factory did not attribute to the wood the problem of the lowest production of tables in the factory, doing so in relation to vitamin D is wrong.What we should do is think how to get vitamin D to have the same effect in patients with autoimmune diseases seems to have in the laboratory .This is exactly what Professor Cícero Coimbra has tried to do over the last few years . To do so, he used the same reasoning as the owner of the now-famous Royal Factory: if one quantifies "what the final result of the vitamin D assembly line", then one can have a true notion of its biological effect on the organism . By achieving this, we can maximize its effect and thereby attempt to replicate the results observed in the laboratory. This leads to the prescription of high doses of vitamin D to achieve the clinical objective of silencing the resulting autoimmune responses of Th17 cells. The first and only studypublished so far shows the possible results with the treatment. In fact, as already mentioned, other works have already been published that follow the same trend. In this study , in Portuguese patients with lupus, vitamin D supplementation showed a decrease in the number of Th17 cells and a better Th17 / Treg ratio . In fact, one of the phrases of the conclusion summarizes the question perfectly:"In spite of displaying optimal circulating vitamin D levels, the ability to metabolize vitamin D may vary between individuals' genetics and thus contribute to the risk of developing immune abnormalities . These conditions are illustrated by the presence of certain gene polymorphisms in the vitamin D metabolizing enzymes, such as CYP2R1 (hydroxylates vitamin D3 to 25 (OH) D in the liver) or CYP27B1 (activated by PTH and hydroxylates 25 (OH) D to 1 , 25 (OH) 2 D 3 in the kidney). Even if all of these steps are properly functioning, the vitamin D active metabolite (1,25 (OH) 2 D 3) must be recognized, bound and activated by its receptor (VDR). Polymorphisms in the VDR gene may also play a role in this mechanism "The complexity is great and there are several steps where imperfections can detract from its function . Even optimal blood levels of vitamin D do not guarantee maximum effectiveness or effectiveness!Ideally, the beneficial action of vitamin D on autoimmunity would be gauged by the decrease in circulating IL17 values or by the number of Th17 or Treg cells produced by the organism . Although they exist, these analyzes are not available for common or clinically wide use: they are only performed in very specialized centers, with high costs. It is necessary to use another mechanism.
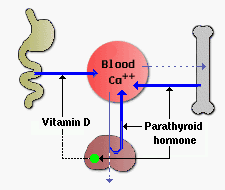
PTH: the effect of vitamin D
Short URL = is.gd/MS20000