Vertigo treated by Vitamin D - many studies
6+ Vitamin D Life pages have VERTIGO or BPPV in the title
Vitamin D Life
Vertigo incidence reduced 40% by just 7,000 IU Vitamin D given weekly - RCT Feb 2024
Common cause of dizziness (BPPV) reduced 5 X by several doses of 50,000 IU of vitamin D – 2015, 2016
Vitamin D may prevent falls by itself – an overview of 9 meta-analysis – Oct 2012
Hearing Loss appears to be prevented and treated with vitamin D
Hearing loss is strongly associated with VertigoDiseases that may be related via low vitamin D
BPPV associated to Osteoporosis could be added due to the first line of the abstract on this pagePreventing Falls in Older Adults – Vitamin D combination is the best - JAMA Meta-analysis Nov 2017
My balance significantly improved at age 73 (perhaps Vitamin D, B12, or Omega-3) – Jan 2020
9+ items on the Web
Role of vitamin D in controlling vertigo: a review - April 2024 FREE PDF
The #1 Vitamin Deficiency Behind Vertigo - Dr. Berg video April 2023
How to Dissolve Crystals in the Inner Ear and Get Rid of Vertigo -Dr. Berg video May 2024
Suspect Vitamin K2 would also be usefulVITAMIN D DEFICIENCY SYMPTOMS & VERTIGO LiveStrong July 2012
- Vitamin D deficiency and low calcium levels in the ear can lead to inner ear dysfunction that includes hearing loss, tinnitus or vertigo
- Your inner ear is partly responsible for your sense of balance, so ear problems may cause dizziness.
- Because vitamin D is necessary for calcium absorption, vitamin D deficiency can lead to osteoporosis and calcium loss in the bones of the inner ear
- How I cured vertigo
- The short answer: To cure vertigo, drink more water and take magnesium.
- Large Vitamin D website in Germany One of the indications of vitamin D deficiency follows:
- Vertigo: I can't see anymore or feel dizzy but I recover when I lie down.
- Vitamin D deficiency and benign paroxysmal positioning vertigo Dec 2012
- [email protected] Hypothesis supported by 4 cured cases
- Low bone mineral density and vitamin D deficiency in patients with benign positional paroxysmal vertigo June 2014
- Nice abstract, but $40 paywall
Canalithiasis form of viertigo has lower vitamin D levels than cupulolithiasis form June 2017, 10.1016/j.bjorl.2017.05.007
The Seasonal Variation of Benign Paroxysmal Positional Vertigo Oct 2016 - 10.1097/MAO.0000000000001534
Vertigo (BPPV) greatly reduced by Vitamin D - meta-analysis April 2025
Association between vitamin D, vitamin D supplementation and benign paroxysmal positional vertigo: a systematic review and meta-analysis
Front Neurol . 2025 Apr 16:16:1560616. doi: 10.3389/fneur.2025.1560616
Yanyan Li # 1, Peng Gao # 2, Rui Ding 3, Ying Xu 1, Zhicheng Wang 1, Xiaorui Pei 1, Lianhe Li 4
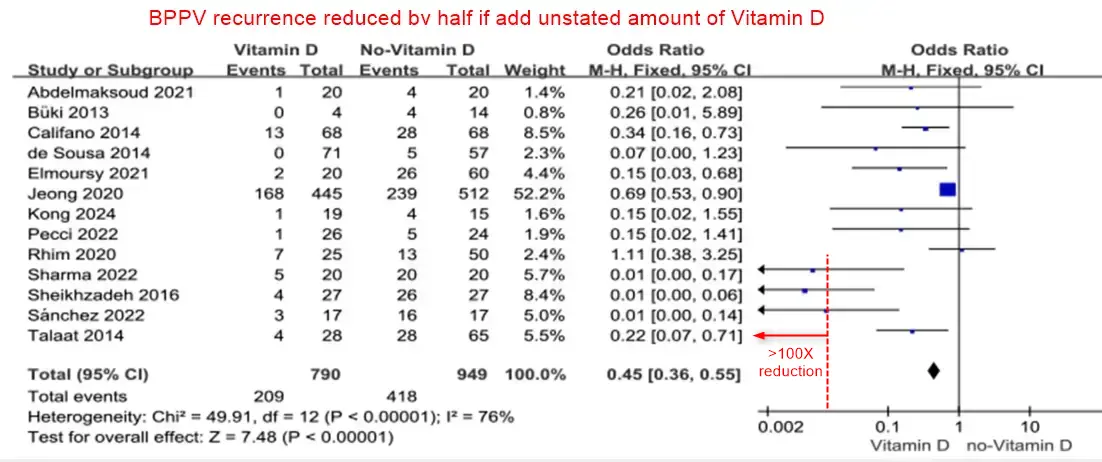
Note: the studies getting >100X reduction are not weighted highly.
Weighting is based only on the number of participants,
not the dose size, dose duration, nor Vitamin D level before the trials started
Background: Benign paroxysmal positional vertigo (BPPV) is one of the most prevalent peripheral vestibular dysfunctions encountered in clinical practice, including dizziness and vertigo, which has a significant impact on people's everyday lives and affects their quality of life in many ways. Researches indicate that individuals with recurrent benign paroxysmal positional vertigo (BPPV) may exhibit vitamin D insufficiency, and certain studies suggest that correcting severe vitamin D deficiency might effectively reduce BPPV recurrence; nevertheless, the findings have been inconsistent. As a result, we conducted the current Meta-analysis to investigate potential associations of vitamin D levels with the occurrence and recurrence of BPPV. In the meantime, the current study was done to evaluate the impact of vitamin D supplementation on the prevention of benign paroxysmal positional vertigo recurrence.
Methods: Electronic databases (PubMed, EMBASE, SCOPUS and the Cochrane Library) were identified to search for relevant studies about (vitamin D or vitamin D supplementation) and (Benign paroxysmal positional vertigo incidence or recurrence) from inception to Dec 22, 2024. 60 studies with a total of 16,368 participants were included into this meta-analysis.
Results:
(1) The aggregated weighted mean difference (WMD) demonstrated that there was a significant reduction in vitamin D level in the BPPV cohort (WMD = -2.84; 95% CI -4.53 to -1.15) relative to the control cohort. Likewise, Recurrent BPPV groups had significantly lower levels of vitamin D compared to non-recurrent groups (WMD = -5.01; 95% CI -6.94 to -3.08). When the cupulolithiasis BPPV groups were compared to the canalolithiasis BPPV groups, the vitamin D level was lower in the cupulolithiasis groups (WMD = 5.09; 95% CI 2.05 to 8.12);
(2) In this meta-analysis, the multivariable-adjusted relative risk (RR) indicated that increased vitamin D was inversely related to BPPV incidence (RR = 1.36; 95% CI 1.31, 1.41), but not significantly related to the recurrence (RR = 0.95, 95% CI 0.91, 0.99);
(3) Vitamin D supplementation group had a lower recurrence rate than the control group which did not accepted vitamin D supplementation (RR =0.45, 95% CI = 0.36-0.55).
Conclusion: The serum level of vitamin D is lower in patients with BPPV, especially recurrent BPPV, than in controls. There was a negative correlation between occurrence rate of BPPV episodes and vitamin D deficiency, which means that vitamin D deficiency may have a role in occurrence of BPPV. The present study indicates that vitamin D supplementation can significantly lower recurrence in benign paroxysmal positional vertigo. The level of vitamin D was lower in canalolithiasis than in cupulolithiasis BPPV groups.
Download the PDF from Vitamin D Life
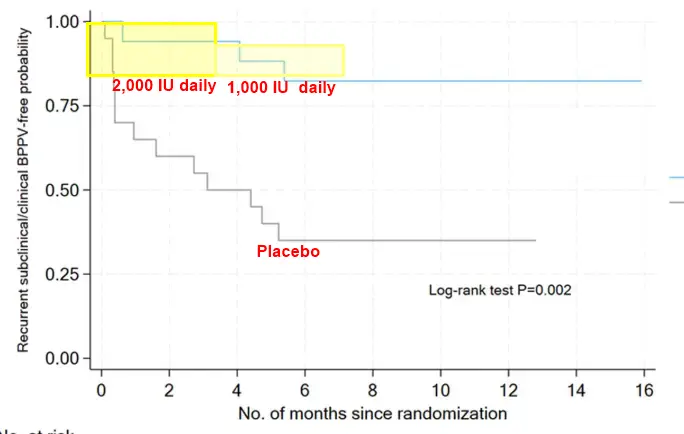
87% reduction in recurrence of BPPV with 13 weeks of Vitamin D (2,000 IU daily) - RCT Aug 2024
Otolaryngol Head Neck Surg. 2024 Aug 28. doi: 10.1002/ohn.954
Randomized Controlled Trial Assessing Vitamin D's Role in Reducing BPPV Recurrence in Older Adults
Kenneth W De Chua 1, Xiaoting Huang 2, Xuan H Koh 3, Joshua F J Y Soh 4, Vivian C Barrera 5, Poongkulali Anaikatti 6, Deng Jing 1, Shirlene Moh 7, Miko Yeo 7, Heng W Yuen 1, David Low 1, Barbara H Rosario 5
Objective: To determine if the recurrence rates of BPPV in older adults were lower in the vitamin D-treated group as compared to placebo groups.
Study design: Double-blinded randomized control placebo trial.
Setting: A single-centre study.
Methods: Double-blinded randomized controlled trial design with 12 months follow-up. Vitamin D3 deplete participants were randomized into treatment ( Group A ) or placebo groups ( Group B ). Treatment group received 13 weeks of 2000 IU vitamin D3 followed by 1000 IU for the next 13 weeks. Patients who were replete were allocated to a control group (Group C) for observation and follow up. All groups had dietary interventions for vitamin D3 and calcium.
Results: Results showed an 87% reduction in recurrence rates of BPPV in the treatment group (Group A), with 0.75 fewer clinical episodes per 1 person-year as compared to placebo ( Group B ). Time to first recurrence was also significantly longer in Group A. There was no statistically significant difference between Group A and C in both recurrence rates and dizziness handicap scores.
Conclusions: This clinical trial has laid the foundation to expand the investigation of vitamin D as standard of care treatment in BPPV patients in future phase IIb and III studies.
Summary: A reduction in BPPV episodes in older adults has implications on fall risk, as dizziness from BPPV may cause falls. With fewer BPPV episodes and longer time to recurrence, seniors may have better postural stability and hence reduced risk of falls.
📄 Download the PDF from Vitamin D Life
BPPV greatly reduced by Vitamin D in those who were deficient – Aug 2024
Evaluating the Vitamin D Deficiency-BPPV Link: Correlation or Causation?
Indian Journal of Otolaryngology and Head & Neck Surgery
https://doi.org/10.1007/s12070-024-04961-9 PDF behind paywall and on DeepDyve
Sanjay Kumar, Anghusman Dutta, Kashiroygoud Biradar & Manish Gupta
Benign Paroxysmal Positional Vertigo (BPPV) is a common vestibular disorder characterized by vertigo episodes due to head position changes. Emerging research suggests a link between Vitamin D deficiency and BPPV, attributed to Vitamin D’s role in calcium metabolism essential for inner ear function. This study investigates the relationship between Vitamin D levels and the incidence, severity, and recurrence of BPPV. This year-long prospective cohort study was conducted at a tertiary care center, enrolling 100 patients diagnosed with BPPV. Vitamin D levels were measured and classified as deficient, insufficient, or sufficient. Patients identified with Vitamin D deficiency (< 20 ng/mL) received supplementation at a dose of 2000 IU daily for six months. Participants were followed monthly for one year to monitor the incidence and severity of BPPV episodes, assessed using the Vertigo Symptom Scale, and recurrence rates. Statistical analysis included Kaplan-Meier curves, log-rank tests, and Cox proportional hazards models to evaluate the Vitamin D-BPPV relationship.
The study revealed that patients with Vitamin D deficiency (< 20 ng/mL) had a 71% incidence of BPPV, compared to 20% in those with sufficient levels. The average severity score was higher in the deficient group (7.5) versus the sufficient group (3.5). Vitamin D supplementation correlated with reduced BPPV incidence and severity over time. The findings indicate a significant link between Vitamin D deficiency and increased BPPV incidence and severity, highlighting Vitamin D’s role in vestibular health. These results suggest that Vitamin D supplementation could be integral to BPPV management. Further research, including controlled studies, is needed to understand the mechanisms behind these associations and their clinical implications.
BPPV recurrences decreased with Vitamin D supplements (4 out of 5 studies) – Feb 2024
Vitamin D Supplementation and Recurrence of Benign Paroxysmal Positional Vertigo
Nutrients. 2024 Feb 28;16(5):689. doi: 10.3390/nu16050689.
Guil Rhim 1, Moon-Jung Kim 2
Positional vertigo manifests as a spinning sensation triggered by changes in head position relative to gravity. Benign paroxysmal positional vertigo (BPPV) is an inner ear disorder characterized by recurrent episodes of positional vertigo. The connection between vitamin D insufficiency/deficiency and the onset and recurrence of BPPV is established. This study aims to assess vitamin D as a recurring factor in BPPV and the efficacy of vitamin D supplementation in preventing its recurrence. A comprehensive literature review on the relationship between vitamin D and BPPV recurrence was conducted, searching PubMed, Embase, Web of Science, and article reference lists for studies published from 2020 to 2023. A total of 79 articles were initially identified through the search, with 12 of them being utilized in the study. Recurrence rates for BPPV varied from 13.7% to 23% for studies with follow-up less than 1 year and 13.3% to 65% for studies with follow-up equal to or exceeding 2 years.
Risk factors for BPPV recurrence include
advanced age,
female sex,
hypertension,
diabetes mellitus,
hyperlipidemia,
osteoporosis, and
vitamin D deficiency.
While earlier studies did not establish a link between low vitamin D levels and initial BPPV occurrence, they did associate recurrent episodes with low vitamin D levels. Recent research indicates that vitamin D supplementation in BPPV patients with deficiency or insufficiency decreases both the numbers of relapsing patients and relapses per patient. To validate these findings across diverse populations, further randomized controlled studies with larger cohorts and extended follow-up durations are essential.
📄 Download the PDF from Vitamin D Life
BPPV associated with low vitamin D - Dr. Berg Video April 2023
The #1 Vitamin Deficiency Behind Vertigo Excellent 9-minute video]
References
https://link.springer.com/article/10.... https://Vitamin D Life.com/tiki-index.p... (This Vitamin D Life page)
https://pubmed.ncbi.nlm.nih.gov/23096...
0:00 Introduction: BPPV explained
0:38 What causes vertigo?
1:15 The Dix-Hallpike test
3:00 The Epley maneuver
4:48 What causes calcium crystals?
7:35 The best remedy for BPPV
He recommends 50,000 IU of vitamin D weekly + Vitamin K2
9:00 Learn more about vitamin D deficiency!
Those still dizzy after BPPV treatment were 5.5 X more likely to have low vitamin D – June 2022
Low 25-Hydroxyvitamin D Levels Are Associated With Residual Dizziness After Successful Treatment of Benign Paroxysmal Positional Vertigo
Front Neurol. 2022 Jun 22;13:915239. doi: 10.3389/fneur.2022.915239. eCollection 2022.
Yunqin Wu 1, Kun Han 1, Weiwei Han 2, Zhenyi Fan 1, Min Zhou 1, Xiaoxiong Lu 1, Xiaoxia Liu 1, Li Li 1, Liwen Du 3
Objective: Vitamin D (Vit D) regulates calcium and phosphate metabolism and helps to maintain otolith organ function. Residual dizziness (RD) is one of the most common complications after the successful treatment of benign paroxysmal positional vertigo (BPPV). Various theories have been suggested to explain the cause of RD, and otolith organ disorder is the most evident cause of RD. This study aimed to investigate the association between serum levels of Vit D and the occurrence of RD after the successful treatment of BPPV.
Methods: A prospective study including patients who were diagnosed with de novo posterior semicircular canal-type BPPV (PC-BPPV) was conducted at our institution from May 2017 to May 2019. All the patients underwent canalith repositioning procedures and were followed up. Univariate and multivariate analyses were performed to investigate the relationship between serum 25-hydroxy vitamin D (25(OH)D) levels and RD occurrence after successful BPPV treatment.
Results: In total, 123 patients with PC-BPPV were enrolled, and 41.5% (51/123) experienced RD . The serum level of 25(OH)D was significantly lower in PC-BPPV patients with RD [median 16.2 ng/ml (IQR 12.9-22.1)] than in patients without RD [median 20.5 ng/ml (IQR 16.5-26.5)] (P = 0.001). In multivariate models comparing the prevalence of RD in the insufficient group [25(OH)D ≥ 20 to <30 ng/ml], deficient group [25(OH)D < 20 ng/ml] and normal group [25(OH)D ≥ 30 ng/ml], the 25(OH)D levels in the deficient group were associated with the occurrence of RD ( odds ratio = 5.48 , 95% confidence interval = 1.08-27.71; P = 0.04).
Conclusion: Low 25(OH)D levels are associated with the development of RD in patients with PC-BPPV after successful treatment. Further efforts to validate and elucidate the mechanism are needed.
📄 Download the PDF from Vitamin D Life
BPPV substantially reduced if raised Vitamin D levels – Aug 2021
Relation between vitamin D deficiency and benign paroxysmal positional vertigo
Sci Rep. 2021 Aug 19;11(1):16855. doi: 10.1038/s41598-021-96445-x.
Aida Ahmed Abdelmaksoud 1, Dalia Fahim Mohammed Fahim 2, Shamardan Ezzeldin Sayed Bazeed 3, Mohamed Farouk Alemam 4, Zaki Farouk Aref 5
📄 Download the PDF from Vitamin D Life

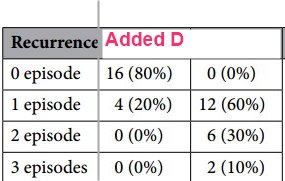
Benign paroxysmal positional vertigo (BPPV) is the most common cause of positional vertigo. Vitamin D deficiency may be one of the causes of its development. To assess the relation between recurrent attacks BPPV and Vitamin D deficiency. A case control study in which 40 patients were clinically diagnosed as posterior canal BPPV, Serum 25(OH) D was measured at 1st visit. Patients were divided into two groups; group A (20 patients) received Vitamin D supplementation in addition to canal repositioning maneuver and group B (20 patients) treated by canal repositioning maneuver only. Follow up of all patients for 6 months, neuro-otological assessment was repeated and recurrent attacks were recorded. Serum vitamin D was repeated after 6 month. This study included 14 males and 26 females age ranged from 35 to 61 years, Average serum of 25 (OH) D at the first visit was (12.4 ± 2 ng/ml) for group A, and (12.2 ± 1.7 ng/ml) for group B, all patients had low serum level of 25(OH) D (below 20 ng/ml). Recurrent BPPV episodes, were significantly lower in group A than that of group B. There is a relation between BPPV recurrence and low serum Vitamin D.
Vitamin D intervention - clipped from PDF
Vitamin D status was classified according to measured 25(OH) D concentration:
less than 10 ng/mL: deficient;
between 11 and 20: insufficient;
For patients with insufficiency and deficiency serum level and no history of nephrolithiasis,
Vitamin D supplement was given in regimen of cholecalciferol
8000 IU daily for 2 weeks, followed by 4000 IU daily for 2 weeks then 8000 IU single dose weekly for 3 months 31
Note: This dosing schedule did not raise Vitamin D levels very much, much more is needed'
References
Gu, X., Dong, F. & Gu, J. Analysis of effect of 1a-hydroxyvitamin D3 on benign paroxysmal positional vertigo and risk factors. Exp. Ther. Med. 15, 2321-2326. https://doi.org/10.3892/etm.2018.5699 (2018).
Neuhauser, H. K. The epidemiology of dizziness and vertigo. Handb. Clin. Neurol. 137, 67-82 (2016).
Neuhauser, H. K. & Lempert, T. Vertigo: Epidemiologic aspects. Semin. Neurol. 29(05), 473-481 (2009).
Parnes, L. S., Agrawal, S. K. & Atlas, J. Diagnosis and management of benign paroxysmal positional vertigo (BPPV). Can. Med. Assoc. J. 169(7), 681-693 (2003).
Nedzelski, J. M., Barber, H. O. & Mcllmoyl, L. Diagnoses in a dizziness unit. J. Otolaryngol. 15(2), 101-104 (1986).
Mohsin, F. D., Alharbawi, F. A. & Alraho, S. T. Benign paroxysmal positional vertigo and vitamin D deficiency. Pharma Innov. J. 8(3), 49-52 (2019).
Bhattacharyya, N. et al. Clinical practice guideline: Benign paroxysmal positional vertigo (update) executive summary. Otolaryngol. Head Neck Surg. 156(3), 403-416. https://doi.org/10.1177/0194599816689660 (2017).
Yang, H. et al. Matrix recruitment and calcium sequestration for spatial specific otoconia development. PLoS ONE6, e20498 (2011).
Lundberg, Y. W., Zhao, X. & Yamoah, E. N. Assembly of the otoconia complex to the macular sensory epithelium of the vestibule. Brain Res. 1091(1), 47-57 (2006).
Lins, U. et al. The otoconia of the guinea pig utricle: Internal structure, surface exposure, and interactions with the filament matrix. J. Struct. Biol. 131, 67-78 (2000).
Lundberg, Y. W., Zhao, X. & Yamoah, E. N. Assembly of the otoconia complex to the macular sensory epithelium of the vestibule. Brain Res. 1091, 47-57 (2006).
Pillai, N. G. & Gopinath, I. A prospective analysis of vitamin D and recurrent benign paroxysmal positional vertigo. Int. J. Otorhi- nolaryngol. Head Neck Surg. 5(6), 1548-1551 (2019).
Zhao, X., Yang, H., Yamoah, E. N. & Lundberg, Y. W. Gene targeting reveals the role of Oc90 as the essential organizer of the otoconial organic matrix. Dev. Biol. 304, 508-524 (2007).
Xu, Y. et al. Expression, functional, and structural analysis of proteins critical for otoconia development. Dev. Dyn. 239, 2659-2673 (2010).
Talaat, H. S., Abuhadied, G., Talaat, A. S. & Abdelaal, M. S. Low bone mineral density and vitamin D deficiency in patients with benign positional paroxysmal vertigo. Eur. Arch. Otorhinolaryngol. 272(9), 2249-2253 (2015).
Buki, B., Ecker, M., Junger, H. & Lundberg, Y. W. Vitamin D deficiency and benign paroxysmal positioning vertigo. Med. Hypotheses. 80(2), 201-204 (2013).
Kudlacek, S. et al. Assessment of vitamin D and calcium status in healthy adult Austrians. Eur. J. Clin. Investig. 33, 323-331 (2003).
Talaat, H. S. et al. Reduction of recurrence rate of benign paroxysmal positional vertigo by treatment of severe vitamin D deficiency. Auris Nasus Larynx 43(3), 237-241 (2016).
Sheikhzadeh, M. et al. Influence of supplemental vitamin D on intensity of benign paroxysmal positional vertigo: A longitudinal clinical study. Casp. J. Intern. Med. 7(2), 93 (2016).
Yu, S., Liu, F., Cheng, Z. & Wang, Q. Association between osteoporosis and benign paroxysmal positional vertigo: A systematic review. BMC Neurol. 14(1), 110 (2014).
Hughes, I., Thalmann, I., Thalmann, R. & Ornitz, D. M. Mixing model systems: Using zebrafish and mouse inner ear mutants and other organ systems to unravel the mystery of otoconial development. Brain Res. 1091(1), 58-74. https://doi.org/10.1016/j.brain res.2006.01.074 (2006).
Bruintjes, T. D., Van der Zaag-Loonen, H. J., Eggelmeijer, F. & Van Leeuwen, R. B. The prevelance of benign positional vertigo in patients with osteoprosis. Eur. Arch. Oto-Rhino-Laryngol. https://doi.org/10.1007/s00405-018-5164-4 (2018).
Kim, S. Y., Kim, H. J., Min, C. & Choi, H. G. Association between benign paroxysmal positional vertigo and osteoporosis: Two nested case-control studies. Osteoporos. Int. 31, 2017-2024 (2020).
Tsiaras, W. G. & Weinstock, M. A. Factors influencing vitamin D status. Acta Derm. Venereol. 91, 115-124 (2011).
Sturges, M. & Canell, J Treating vitamin D deficiency may help reduce the recurrence rate of vertigo, according to study Posted on (2015).
Weir, N. Sensorineural deafness associated with recessive hypophosphataemic rickets. J. Laryngol. Otol. 91, 717-722 (1977).
Brookes, E. B. & Morrison, A. W. Vitamin D deficiency and deafness. Br. Med. J. (Clin. Res. Ed.) 283, 273-274 (1981).
Von Brevern, M. et al. Benign paroxysmal positional vertigo: Diagnostic criteria Consensus document of the Committee for the Classification of Vestibular Disorders of the Barany Society. J. Vestib. Res. 25, 105-117. https://doi.org/10.3233/VES-150553 (2015).
Dhameliya, J. D., Chandra, U. K., Vishwakarma, S. K., Ganganpalli, D. & Verma, A. Investigating the association between serum vitamin D deficiency and idiopathic benign paroxysmal positional vertigo. Int. Clin. Neurosci. J. 7(3), 122-126. https://doi.org/10.34172/icnj.2020.12 (2020).
Souberbielle, J. C. et al. Vitamin D and musculoskeletal health, cardiovasculardisease, autoimmunity and cancer: Recommendations for clinical practice. Autoimmun. Rev. 9, 709-715 (2010).
Thacher, T. D. & Clarke, B. L. Vitamin D insufficiency. Mayo Clin. Proc. 86, 50-60 (2011).
Saeed, B. M. N. & Omari, A. F. Climatic variations and benign paroxysmal positional vertigo. J. Otol. 11, 33-37 (2016).
Zuma E Maia F. C., de Fraga, R. B., Ramos, B. F., Cal, R. V. & Mangabeira Albernaz, P. L. Seasonality and solar radiation variation level in benign paroxysmal positional vertigo. Acta. Otol.. 139(6), 497-499. https://doi.org/10.1080/00016489.2019.1590636 (2019).
Rhim, L. G. Serum vitamin D and long-term outcomes of benign paroxysmal positional vertigo. Clin. Exp. Otorhinolaryngol. 12(3), 273-278 (2019).
Mithal, A. et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 20, 1807-1820. https://doi.org/10.1007/s00198-009-0954-6 (2009).
Sakaida, M., Takeuchi, K., Ishinaga, H., Adachi, M. & Majima, Y. Long-term outcome of benign paroxysmal positional vertigo. Neurology 60(9), 1532-1534 (2003).
Brandt, T., Huppert, D., Hecht, J., Karch, C. & Strupp, M. Benign paroxysmal positioning vertigo: A long-term follow-up (6-17 years) of 125 patients. Acta Otolaryngol. 126(2), 160-163 (2006).
Tanimoto, H., Doi, K., Nishikawa, T. & Nibu, K. Risk factors for recurrence of benign paroxysmal positional vertigo. J. Otolaryngol. Head Neck Surg. 37(6), 832-835 (2008).
Rhim, G. I. Serum vitamin D and recurrent benign paroxysmal positional vertigo. Laryngosc. Investig. Otolaryngol. 1(6), 150-153 (2016).
Vibert, D., Kompis, M. & Hausler, R. Benign paroxysmal positional vertigo in older women may be related to osteoporosis and osteopenia. Ann. Otol. Rhinol. Laryngol. 112, 885-889 (2003).
Yamanaka, T. et al. Osteoporosis as a risk factor for the recurrence of benign paroxysmal positional vertigo. Laryngoscope. 123(11), 2813-2816 (2013).
Jeong, S. H. et al. Decreased serum vitamin D in idiopathic benign paroxysmal positional vertigo. J. Neurol. 260(3), 832-838 (2013).
Vertigo associated with low vitamin D, supplementation reduced relapse (PDF costs $36) - Nov 2021
The role of low levels of vitamin D as a co-factor in the relapse of benign paroxysmal positional vertigo (BPPV)
Am J Otolaryngol . 2021 Jun 19;42(6):103134. doi: 10.1016/j.amjoto.2021.103134
Mohamed Mohamed Elmoursy 1, Awad Saad Abbas 2
Background: Benign paroxysmal positional vertigo is characterized as brief episodes of vertigo that are exacerbated by the unexpected act of moving to a current provoking location. It is thought to be an otoconia-related balance disorder. Our objectives were to assess the serum concentrations of vitamin D and calcium (total and ionized) in cases with BPPV, determine if low vitamin D levels were regarded as a cause for BPPV relapse, and determine whether vitamin D supplementation would minimize the risk of BPPV relapse.
Results: Sixty cases with BPPV were included in the study; 53 cases had posterior canal BPPV, while seven had lateral canal BPPV. Canalithiasis was the most common type of BPPV pathology. Forty cases had abnormally low levels of vitamin D. There was a statistically significant positive correlation between the mean vitamin D assay for all cases with BPPV and serum calcium. There was statistically significant difference in comparing the relapse of BPPV for group that receive vitamin D after one year follow up.
Conclusion: Abnormal vitamin D levels were linked with the incident and relapse of BPPV.
Correction of low vitamin D levels was linked with the reduction of the relapse of BPPV
BPPV somewhat reduced by just 800 IU of Vitamin D + Calcium - RCT Aug 2020
Prevention of Benign Paroxysmal Positional Vertigo with Vit D Supplementation: A Randomized Trial
DOI: https://doi.org/10.1212/WNL.0000000000010343
Overview and some details on Medscape no placebo, just a control group
"The dislodgment of particles in the ears called otoconia is thought to initiate these attacks."
"The number of recurrences per one-person year was 0.83 in the intervention group and 1.10 in the observation group. This yielded an incidence rate ratio (IRR) of 0.76 and a reduction in the annual recurrence rate of 0.27 with supplementation. The preventive effect was even more pronounced among patients with decreased serum vitamin D of less than 20 ng/mL at baseline."
"Among treated patients, serum vitamin D levels increased from 13.3 ng/mL at baseline to 24.4 ng/mL at 2 months and 24.2 ng/mL at 1 year."
- Note by Vitamin D Life - clearly the RCT should have used larger doses (to get > 30 ng)
BPPV has many risk factors, low Vitamin D is one of them – Meta-analysis Aug 2020
Risk factors for benign paroxysmal positional vertigo recurrence: a systematic review and meta-analysis
Review J Neurol. 2020 Aug 24. doi: 10.1007/s00415-020-10175-0
Jinbao Chen 1, Senlin Zhang 2, Kai Cui 2, Chuxuan Liu 3
📄 Download the PDF from sci-hub via Vitamin D Life
Background and purpose: Benign paroxysmal positional vertigo is one of the most common vestibular diseases, especially in the elderly. Although the treatment of BPPV is relatively successful, many patients suffer recurrence after treatment. Therefore, identifying potential risk factors for BPPV recurrence may help improve treatment outcome and patient prognosis. However, some related risk factors for BPPV recurrence are relatively controversial and poorly studied. This meta-analysis aims to identify potential risk factors associated with BPPV recurrence, thereby reducing the recurrence rate of BPPV and improving the prognosis of patients.
Methods: This meta-analysis was conducted through systematically searching PubMed, Embase, and the Cochrane Library for eligible English original studies published up to June 2020. All search results were reviewed based on our inclusion and exclusion criteria. We calculated the pooled odds ratios (ORs) or the mean differences (MDs) with their corresponding 95% confidence intervals (CIs) to evaluate the effects of included risk factors on BPPV recurrence.
Results: A total of 14 studies involving 3060 BPPV patients published between 2010 and 2019 were finally included, including six prospective studies and eight retrospective studies, with a NOS score ranged from 6 to 9. Our pooled results of this meta-analysis suggested that the recurrence of BPPV was closely related to
female gender (OR = 1.42; 95% CI 1.17-1.74; P = 0.0004),
hypertension (OR = 2.61; 95% CI 1.22-5.59; P = 0.01),
diabetes mellitus (OR = 2.62; 95% CI 1.25-5.48; P = 0.01),
hyperlipidemia (OR = 1.60; 95% CI 1.23-2.09; P = 0.0006),
osteoporosis (OR = 1.72; 95% CI 1.03-2.88; P = 0.04) and
vitamin D deficiency (MD = - 3.29; 95% CI - 5.32 to - 1.26; P = 0.001).
Conclusion: This meta-analysis indicated that female gender, hypertension, diabetes mellitus, hyperlipidemia, osteoporosis, and vitamin D deficiency were risk factors for BPPV recurrence. However, the effects of other potential risk factors including advanced age, migraine, head trauma, and Menière's disease on BPPV recurrence need further investigations. Furthermore, most studies included in this meta-analysis were performed in Asia, so our results cannot easily be extended to the whole world population. Therefore, more large-scale prospective studies in different countries are required to further investigate these risk factors.
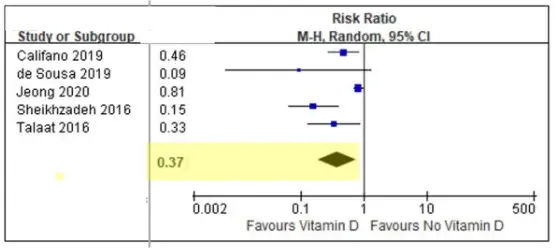
BPPV risk reduced 3X with Vitamin D - meta-analysis Aug 2020
Prevention of recurrent benign paroxysmal positional vertigo with vitamin D supplementation: a meta-analysis
Journal of Neurology Volume 269, pages 619–626, (2022) https://doi.org/10.1007/s00415-020-09952-8 PDF behind paywall
Seong-Hae Jeong, Sun-Uk Lee & Ji-Soo Kim
Research Background
Vitamin D insufficiency/deficiency is known to be related to occurrences and recurrences of benign paroxysmal positional vertigo (BPPV). However, the efficacy of vitamin D supplementation in reducing recurrences of BPPV remains to be established. We performed a meta-analysis to determine the therapeutic effects of vitamin D supplementation, with or without calcium, for preventing recurrences of BPPV.
Methods
We searched the PubMed, the Embase, the Web of Science and the reference lists of the articles. We included randomized or non-randomized trials that determined the efficacy of supplementing vitamin D or related compounds, alone or with calcium, in comparison to placebo or no intervention in preventing recurrences of BPPV. The primary outcome was the number of patients with BPPV recurrences. Data were collected and pooled using a weighted relative risk (RR) with corresponding 95% CIs, where possible, by adopting the fixed-effect or random-effect model according to the heterogeneity among the studies. The between-study heterogeneity was tested using the χ2 test and the I2 statistic, and funnel plots were used to evaluate any publication bias.
Results
We included five trials (four non-randomized trials and one randomized controlled trial) with a total of 1250 participants. The analyses showed a significant preventive effect on the recurrences of BPPV (RR = 0.37; 95% CI = 0.18–0.76; p = 0.007 with the random-effects model) with supplementation of vitamin D. Although a considerable heterogeneity was detected among the studies, the sensitivity analyses showed the reliability and stability of our results.
Conclusions
Vitamin D supplementation provides a benefit for secondary prevention of BPPV. Supplementation of vitamin D should be considered in patients with frequent attacks of BPPV, especially when serum vitamin D is subnormal.
BPPV 2X more likely if low Vitamin D - meta-analysis of 18 studies Jan 2020
Association Between Serum Vitamin D Levels and Benign Paroxysmal Positional Vertigo: A Systematic Review and Meta-Analysis of Observational Studies
Eur Arch Otorhinolaryngol, 277 (1), 169-177 Jan 2020, PMID: 31630244 DOI: 10.1007/s00405-019-05694-0
Baiyuan Yang 1, Yongxia Lu 2, Dongmei Xing 3, Wei Zhong 1, Qing Tang 1, Jingyu Liu 2, Xinglong Yang 4
Objective: Benign paroxysmal positional vertigo (BPPV) was the most common neuro-otological disorder manifests as recurrent positional vertigo, but its risk factors are elusive. Recent studies suggest that decreased Vitamin D level may be a risk factor, but the literature is inconsistent.
Methods: The databases PubMed, Web of Science, Chinese National Knowledge Infrastructure, Wanfang, SinoMed, and Embase were systematically searched for studies on the association between BPPV and serum Vitamin D levels published up to June 2019. Data from eligible studies were meta-analyzed using Stata 12.0.
Results: A total of 18 studies were included in the analysis. Serum Vitamin D levels were significantly lower in individuals with BPPV than in controls (WMD - 2.46, 95% CI - 3.79 to - 1.12, p < 0.001). Subgroup analysis by geographical area showed that vitamin D level was significantly lower in BPPV than in controls in China (WMD - 3.27, 95% CI - 4.12 to - 2.43, p < 0.001), but not outside China (WMD - 0.90, 95% CI - 4.36 to 2.56, p = 0.611). Vitamin D levels were significantly lower in recurrent than non-recurrent BPPV across all countries in the sample (WMD 2.59, 95% CI 0.35-4.82, p = 0.023). Vitamin D deficiency emerged as an independent risk factor of BPPV (OR 1.998, 95% CI 1.400-2.851, p < 0.001).
Conclusion: The available evidence suggests that BPPV is associated with decreased levels of serum Vitamin D, and vitamin D deficiency was an independent risk factor for BPPV.
Vitamin D is associated with BPPV - meta-analysis Oct 2019
Association between serum vitamin D levels and benign paroxysmal positional vertigo: a systematic review and meta-analysis of observational studies
European Archives of Oto-Rhino-Laryngology volume 277, pages169–177 (2020) https://doi.org/10.1007/s00405-019-05694-0
Baiyuan Yang, Yongxia Lu, Dongmei Xing, Wei Zhong, Qing Tang, Jingyu Liu & Xinglong Yang
Objective
Benign paroxysmal positional vertigo (BPPV) was the most common neuro-otological disorder manifests as recurrent positional vertigo, but its risk factors are elusive. Recent studies suggest that decreased Vitamin D level may be a risk factor, but the literature is inconsistent.
Methods
The databases PubMed, Web of Science, Chinese National Knowledge Infrastructure, Wanfang, SinoMed, and Embase were systematically searched for studies on the association between BPPV and serum Vitamin D levels published up to June 2019. Data from eligible studies were meta-analyzed using Stata 12.0.
Results
A total of 18 studies were included in the analysis. Serum Vitamin D levels were significantly lower in individuals with BPPV than in controls (WMD − 2.46, 95% CI − 3.79 to − 1.12, p < 0.001). Subgroup analysis by geographical area showed that vitamin D level was significantly lower in BPPV than in controls in China (WMD − 3.27, 95% CI − 4.12 to − 2.43, p < 0.001), but not outside China (WMD − 0.90, 95% CI − 4.36 to 2.56, p = 0.611). Vitamin D levels were significantly lower in recurrent than non-recurrent BPPV across all countries in the sample (WMD 2.59, 95% CI 0.35–4.82, p = 0.023). Vitamin D deficiency emerged as an independent risk factor of BPPV (OR 1.998, 95% CI 1.400–2.851, p < 0.001).
Conclusion
The available evidence suggests that BPPV is associated with decreased levels of serum Vitamin D, and vitamin D deficiency was an independent risk factor for BPPV.
📄 Download the PDF from Vitamin D Life
BPPV eliminated by Vitamin D – April 2019
Vitamin D deficiency and benign paroxysmal positioning vertigo
Journal of Hearing, Balance, and Communication doi.org/10.1080/21695717.2019.1590988
Pedro Jorge Matos Carneiro de Sousa, Diogo Manuel Abreu Pereira, Pedro Carneiro Melo Pereira de Magalhães, Delfim Rui da Silva Duarte & Nuno Maria Trigueiros da Silva Cunha
📄 Download the PDF from Sci-Hub via Vitamin D Life
Treatment group - NO Vertigo
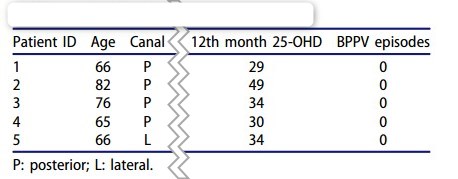
Objectives: Benign paroxysmal positioning vertigo (BPPV) has significant recurrence rates, mainly in older patients. The etiopathology of recurrent BPPV is possibly related to low serum vitamin D levels. Finding a therapeutic weapon will help with these complicated cases, reducing disability, falling risk and also health care costs.
Study design: Clinical trial: one-year duration.
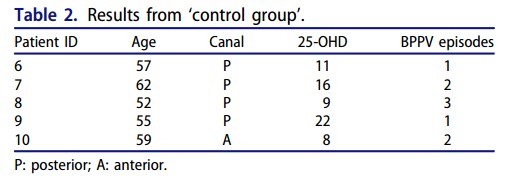
Setting: Ten patients with diagnosis of BPPV made by history and physical examination and at least two episodes of documented BPPV in the previous two years and chronic complaints of dizziness. Neurologic and other otological diseases were excluded for these patients.
Subjects and methods: Vitamin D was evaluated by measuring serum 25-hydroxyvitamin D (25-OHD). Levels below 20 ng/mL were considered deficiency and levels between 20 and 30 ng/mL were considered insufficiency. Half of the patients (treatment group) started a treatment with cholecalciferol while the remaining patients were the control group. All of the patients were reevaluated every three months.
Results: All patients of the treatment group did not have any subsequent episode of positional vertigo, dizziness complaints or nystagmus evoked by provocative manoeuvers. At reevaluations, the mean value of serum 25-OHD for the treatment group had increased noticeably. It was also significantly higher than the mean value of control group. All patients of control group had positional vertigo episodes, as well as positional nystagmus at office reevaluations.
Conclusion: These results support the need to systematically measure and correct vitamin D levels in patients with recurrent BPPV.
BPPV Meta-analysis found no association with low vitamin D in the blood- Oct 2018
Association of benign paroxysmal positional vertigo with vitamin D deficiency: a systematic review and meta-analysis
https://doi.org/10.1007/s00405-018-5146-6 7 studies
Conclusion: "Although a negative vitamin D imbalance has been reported among some BPPV patients, this review analysis failed to establish a relationship between the occurrence of BPPV and low vitamin D level. However, low vitamin D level was significantly evident among patients with recurrent episodes of BPPV."
Vitamin D Life: Meta-analysis seems to ignore the possibility that there is an OK level of vitamin D in the blood, and that Vitamin D is not getting to the cells of the ear due to poor gene activation.
Calcium Carbonate crystals in ear decrease in elderly with low Vit D - April 2018
A Relationship Between Blood Levels of Otolin-1 and Vitamin D
"There was a negative correlation between vitamin D and otolin-1 levels of subjects over 70 (r = -0.36, p = 0.036)."
CONCLUSION: "Our results demonstrate a relationship between vitamin D and otolin-1. The majority of our subjects had abnormally low vitamin D levels, but only those over 70 years of age showed a negative correlation with high otolin-1 levels. We postulate that a seasonal drop in vitamin D may not be sufficient for otoconia fragmentation and ultimately iBPPV; rather, chronically low vitamin D may be required to induce otoconia degeneration."
- DOI: 10.1097/MAO.0000000000001747
BPPV 23X more likely if vitamin D deficient - Oct 2012
Decreased serum vitamin D in idiopathic benign paroxysmal positional vertigo - Oct 2012
J Neurol. 2012 Oct 25.
Jeong SH, Kim JS, Shin JW, Kim S, Lee H, Lee AY, Kim JM, Jo H, Song J, Ghim Y.
Department of Neurology, Chungnam National University College of Medicine, Chungnam National University Hospital, Daejeon, Korea.
Previous studies have demonstrated an association of osteopenia/osteoporosis with idiopathic benign paroxysmal positional vertigo (BPPV). Since vitamin D takes part in the regulation of calcium and phosphorus found in the body and plays an important role in maintaining proper bone structure, decreased bone mineral density in patients with BPPV may be related to decreased serum vitamin D. We measured the serum levels of 25-hydroxyvitamin D in 100 patients (63 women and 37 men, mean age ± SD = 61.8 ± 11.6) with idiopathic BPPV and compared the data with those of 192 controls (101 women and 91 men, mean age ± SD = 60.3 ± 11.3) who had lived in the same community without dizziness or imbalance during the preceding year. The selection of the controls and acquisition of clinical information were done using the data from the Fourth Korean National Health and Nutrition Examination Survey, 2008.
The serum level of 25-hydroxyvitamin D was lower in the patients with BPPV than in the controls (mean ± SD = 14.4 ± 8.4 versus 19.1 ± 6.8 ng/ml, p = 0.001). Furthermore, patients with BPPV showed a higher prevalence of decreased serum vitamin D (<20 ng/ml, 80.0 vs. 60.1 %, p < 0.001) than the controls.
Multiple logistic regression analyses adjusted for age, sex, body mass index, hypertension, diabetes, proteinuria, regular exercise and the existence of decreased bone mineral density demonstrated that vitamin D insufficiency (10-20 ng/ml) and deficiency (<10 ng/ml) were associated with BPPV with the odds ratios of 3.8 (95 % confidence interval = 1.51-9.38, p = 0.004) and 23.0 (95 % confidence interval = 6.88-77.05, p < 0.001). Our study demonstrated an association between idiopathic BPPV and decreased serum vitamin D. Decreased serum vitamin D may be a risk factor of BPPV.
__#00F:Vitamin D Life comment: Perhaps additional possible suspects are low Magnesium and low Vitamin K2'' **---
BPPV reduced 5 X by 50,000 IU of vitamin D every 2 weeks - 2016* The effect of serum vitamin D normalization in preventing recurrences of benign paroxysmal positional vertigo: A case-control study. *Caspian J Intern Med. 2016 Summer;7(3):173-177.
Sheikhzadeh M1, Lotfi Y1, Mousavi A2, Heidari B3, Bakhshi E4.
METHODS: Diagnosis of BPPV was made based on history and clinical examination and exclusion of other conditions. Serum 25-hydroxy vitamin D (25-OHD) was measured using ELISA method and a levels of < 20 ng/ml was considered a deficiency of vitamin D. Inclusion criteria were as follows: history of recurrent attacks and serum 25-OHD<20.ng/ml. While the patients with history of trauma, surgery and chronic systemic diseases were excluded. The patients were classified into two groups: treatment and control, intermittently. Both groups received Epley rehabilitation therapy one session per week for 4 weeks but the treatment group received an additional supplement of 50.000 IU of vitamin D (cholecalciferol) weekly for two months to achieve serum 25-OHD ≥ 30 ng/ml and the study patients were followed-up for 6 months.
RESULTS: Twenty-seven patients were allocated to each group. At baseline, serum 25-OHD was similar (10.7±2.3 vs 11.41±1.9, P=0.23). At month 2, serum 25-OHD in the treatment group increased significantly to ≥ 30 ng/ ml, whereas serum 25-OHD in the control group remained unchanged (34.2±3.3 vs 10.6 10.6±2.2 ng/ml, P=0.001). During the follow-up period, attacks of BPPV in the treatment group decreased significantly compared with the control group (14.8% vs 96.3%* OR= 0.18 *, P=0.001).
CONCLUSION: The findings of this study indicate that the normalization of serum vitamin D significantly reduces BPPV recurrences.
BPPV 2.1 X more likely if low vitamin D - Dec 2017
Note: the 2012 study looked at#00F:* benign paroxysmal positional vertigo Low 25-hydroxyvitamin D levels in postmenopausal female patients with benign paroxysmal positional vertigo Dec 2017 10.1080/00016489.2017.1416168 {FONT( size="16")} 📄 PDF from Sci-Hub via Vitamin D Life *{FONT}
BPPV much more common with low vitamin D - Oct 2016* Serum vitamin D and recurrent benign paroxysmal positional vertigo. *Laryngoscope Investig Otolaryngol. 2016 Oct 20;1(6):150-153. doi: 10.1002/lio2.35. eCollection 2016 Dec.
Rhim GI1.
OBJECTIVES: The objective of the present study was to examine the effects of serum 25-hydroxyvitamin D concentrations on patients diagnosed with benign paroxysmal positional vertigo (BPPV) on BPPV recurrence.
STUDY DESIGN: Case series.
METHODS: A retrospective review of 232 patients diagnosed with BPPV visiting the clinic between June 2014 and June 2015 was performed. All patients underwent a complete otolaryngological, audiologic, and neurologic evaluation. The appropriate particle-repositioning maneuver was performed depending on the type of BPPV. The patients were divided into the recurrence group and the nonrecurrence group. Age, gender, follow-up period, type of BPPV, and vitamin D concentrations in the two groups were compared and analyzed through binary logistic regression analyses.
RESULTS: The average follow-up period after treatment was 10.2 months. Forty-one (17.7%) of 232 patients suffered a recurrence during the follow-up period. The mean vitamin D concentration of 191 patients who did not suffer any recurrence was 16.63 ng/mL, whereas that of 41 patients who suffered a recurrence was 13.64 ng/mL. This difference in vitamin D concentrations was statistically significant (P < 0.019). The patients' age, gender, follow-up period, and type of BPPV had no statistically significant impact.
CONCLUSION: Vitamin D is assumed to affect BPPV as a recurrence factor independent of age, gender, follow-up period, and type of BPPV.
LEVEL OF EVIDENCE: 4.* 📄 Download the PDF from Vitamin D Life * Possible reasons for association - clipped from PDF "The authors (of another study) presented two mechanisms of the relationships between BPPV and osteopenia or osteopenia * First, the decrease of estrogen in reducing the natural regulators of bone mass might disturb the internal structure of the otoconia and/or their interconnection and attachment to the gelatinous matrix.
- Second, an increase of calcium resorption might generate increased concentration of free calcium in the endolymph and reduce its capacity to dissolve the dislodged otoconia."
Semont maneuver eliminates BPPV in 70% to 90% of people (removes crystals from ear (nothing about vitamin D)
{FONT(size="17")}** 📄 Download the PDF from Vitamin D Life {FONT} In June 2025 a single treatment cured my wife of BPPV that she had for months__