Vitamin D Global Perspective - Holick
Mayo Clinic Proceedings, Volume 88, Issue 7 , Pages 720-755, July 2013
Arash Hossein-nezhad, MD, PhD, and Michael F. Holick, PhD, MD
PDF is attached at the bottom of this page
See also recent by Holick on Vitamin D Life
Search Vitamin D Life with Holick in the title 40 pages as of Dec 2015
It is now generally accepted that vitamin D deficiency is a worldwide health problem that affects not only musculoskeletal health but also a wide range of acute and chronic diseases. However, there remains cynicism about the lack of randomized controlled trials to support the association studies regarding the nonskeletal health benefits of vitamin D. This review was obtained by searching English-language studies published up to April 1, 2013, in PubMed, MEDLINE, and the Cochrane Central Register of Controlled Trials (search terms: vitamin D and supplementation) and focuses on recent challenges regarding the definition of vitamin D deficiency and how to achieve optimal serum 25-hydroxyvitamin D concentrations from dietary sources, supplements, and sun exposure. The effect of vitamin D on fetal programming epigenetics and gene regulation could potentially explain why vitamin D has been reported to have such wide-ranging health benefits throughout life. There is potentially a great upside to increasing the vitamin D status of children and adults worldwide for improving musculoskeletal health and reducing the risk of chronic illnesses, including some cancers, autoimmune diseases, infectious diseases, type 2 diabetes mellitus, neurocognitive disorders, and mortality.
Vitamin D deficiency has been recognized as a pandemic with a myriad of health consequences.1,2 Low vitamin D status has been associated with an increased risk of type 1 diabetes mellitus, cardiovascular disease, certain cancers, cognitive decline, depression, pregnancy complications, autoimmunity, allergy, and even frailty.1-4 Low prenatal and neonatal vitamin D status may also increase susceptibility to schizophrenia, type 1 diabetes, and multiple sclerosis (MS) in later life via specific target organ effects, including the immune system, or through epigenetic modification.5
Despite the many important health benefits of vitamin D, there is controversy regarding the definition of vitamin D deficiency and what the vitamin D requirement should be.2,6,7 In addition, critical windows of exposure to adequate vitamin D levels during fetal maturation remain to be defined5,6 owing, in part, to the lack of well-designed controlled clinical trials with long-term follow-up.5-7
This review, obtained, in part, from searching English-language studies published up to April 1, 2013, in PubMed, MEDLINE, and the Cochrane Central Register of Controlled Trials (search terms: vitamin D and supplementation), focuses on recent challenges about how to achieve an optimal serum level of 25-hydroxyvitamin D [25(OH)D] from dietary sources, supplements, and sun exposure and evidence-based benefits for skeletal and nonskeletal health. Also, we explore fetal programming and epigenomic mechanisms that could potentially explain why vitamin D has been reported to have such wide-ranging health benefits throughout life.
ARTICLE HIGHLIGHTS
Vitamin D deficiency is a common underdiagnosed condition.
Recent evidence from hundreds of studies suggests that vitamin D is important for reducing the risk of
- type 1 diabetes mellitus, cardiovascular disease, certain cancers, cognitive decline, depression, pregnancy complications, autoimmunity, allergy, and even frailty.
The blood level of 25(OH)D is the best method to determine vitamin D status.
Vitamin D deficiency during pregnancy may influence fetal "imprinting" that may affect chronic disease susceptibility soon after birth as well as later in life.
An effective strategy to prevent vitamin D deficiency and insufficiency is to obtain some sensible sun exposure, ingest foods that contain vitamin D, and take a vitamin D supplement.
VITAMIN D METABOLISM AND BIOLOGICAL FUNCTIONS
Vitamin D (D represents D2,D3, or both) is a secosterol produced endogenously in the skin from sun exposure or obtained from foods that naturally contain vitamin D, including cod liver oil and fatty fish (eg, salmon, mackerel, and tuna); UV-irradiated mushrooms; foods fortified with vitamin D; and supplements.2,7 During exposure to sunlight, 7-dehydro-cholesterol (7-DHC) in the skin is converted to previtamin D3. The 7-DHC is present in all the layers of human skin.7-9 Approximately 65% of 7-DHC is found in the epidermis, and greater than 95% of the previtamin D3 that is produced is in the viable epidermis and, therefore, cannot be removed from the skin when it is washed.9 Once previtamin D3 is synthesized in the skin, it can undergo either a photoconver-sion to lumisterol, tachysterol, and 7-DHC or a heat-induced membrane-enhanced isomerization to vitamin D3 (Figure 1).7,8 The cutaneous production of previtamin D3 is regulated. Solar photoproducts (tachysterol and lumisterol) inactive on calcium metabolism are produced at times of prolonged exposure to solar UV-B radiation, thus preventing sun-induced vitamin D intoxication.7,8 Vitamin D3 is also sensitive to solar irradiation and is, thereby, inactivated to suprasterol 1 and 2 and to 5,6-trans-vitamin D3.7 Cutaneous vitamin D3 production is influenced by skin pigmentation, sunscreen use, time of day, season, latitude, altitude, and air pollution.1,2,7,8 An increase in the zenith angle of the sun during winter and early morning and late afternoon results in a longer path for the solar UV-B photons to travel through the ozone layer, which efficiently absorbs them. This is the explanation for why above and below approximately 33° latitude little if any vitamin D3 is made in the skin during winter.10,11 This is also the explanation for why—whether being at the equator and in the far northern and southern regions of the world in summer, where the sun shines almost 24 hours a day—vitamin D3 synthesis occurs only between approximately 10 AM and 3 pm.1,11 Similarly, in urban areas, such as Los Angeles, California, and Mexico City, Mexico, where nitrogen dioxide and ozone levels are high, few vitamin D3—producing UV-B photons reach the people living in these cities.7,11 Similarly, because glass absorbs all UV-B radiation, no vitamin D3 is produced in the skin when the skin is exposed to sunlight that passes through glass.
Once formed, vitamin D3 is ejected out of the keratinocyte plasma membrane and is drawn into the dermal capillary bed by the vitamin D binding protein (DBP).7,8 Vitamin D that is ingested is incorporated into chylomicrons, which are released into the lymphatic system, and enters the venous blood,2,7 where it binds to DBP and lipoproteins transported to the liver.1,2,7 Vitamin D2 and vitamin D3 are 25-hydroxylated by the liver vitamin D-25-hydroxylase (CYP2R1) to produce the major circulating vitamin D metabolite, 25(OH)D, which is used to determine a patient's vitamin D status.1,2,7 This metabolite undergoes further hydroxylation by the 25(OH)D-1a-hy-droxylase (CYP27B1) in the kidneys to form the secosteroid hormone 1a,25-dihydroxyvitamin D [1,25(OH)2D] (Figure1).2,7,12 The 25(OH)D bound to DBP is filtered in the kidneys and is reabsorbed in the proximal renal tubules by megalin cubilin receptors.6,12
The renal 1 a-hydroxylation is closely regulated, being enhanced by parathyroid hormone (PTH), hypocalcemia, and hypophosphatemia and inhibited by hyperphosphatemia, fibroblast growth factor-23, and 1,25(OH)2D itself.7,13,14 The 1,25(OH)2D performs many of its biologic functions by regulating gene transcription through a nuclear high-affinity vitamin D receptor (VDR).15,16 This active metabolite of vitamin D binds to the nuclear VDR, which binds retinoic acid X receptor to form a hetero-dimeric complex that binds to specific nucleo-tide sequences in the DNA known as vitamin D response elements. Once bound, a variety of transcription factors attach to this complex, resulting in either up-regulation or down-regulation of the gene's activity.2,7,17 There are estimated to be 200 to 2000 genes that have vitamin D response elements or that are influenced indirectly, possibly by epigenetics, to control a multitude of genes across the genome.2,16 A recent microarray study on the influence of vitamin D status and vitamin D3 supplementation on genome-wide expression in white blood cells before and after vitamin D3 supplementation found that an improved serum 25(OH)D concentration was associated with at least a 1.5-fold alteration in the expression of 291 genes.17 This study suggested that any improvement in vitamin D status will significantly affect the expression of genes that have a variety of biologic functions of more than 80 pathways linked to cancer, autoimmune disorders, and cardiovascular disease, which have been associated with vitamin D deficiency.17
FIGURE 1.
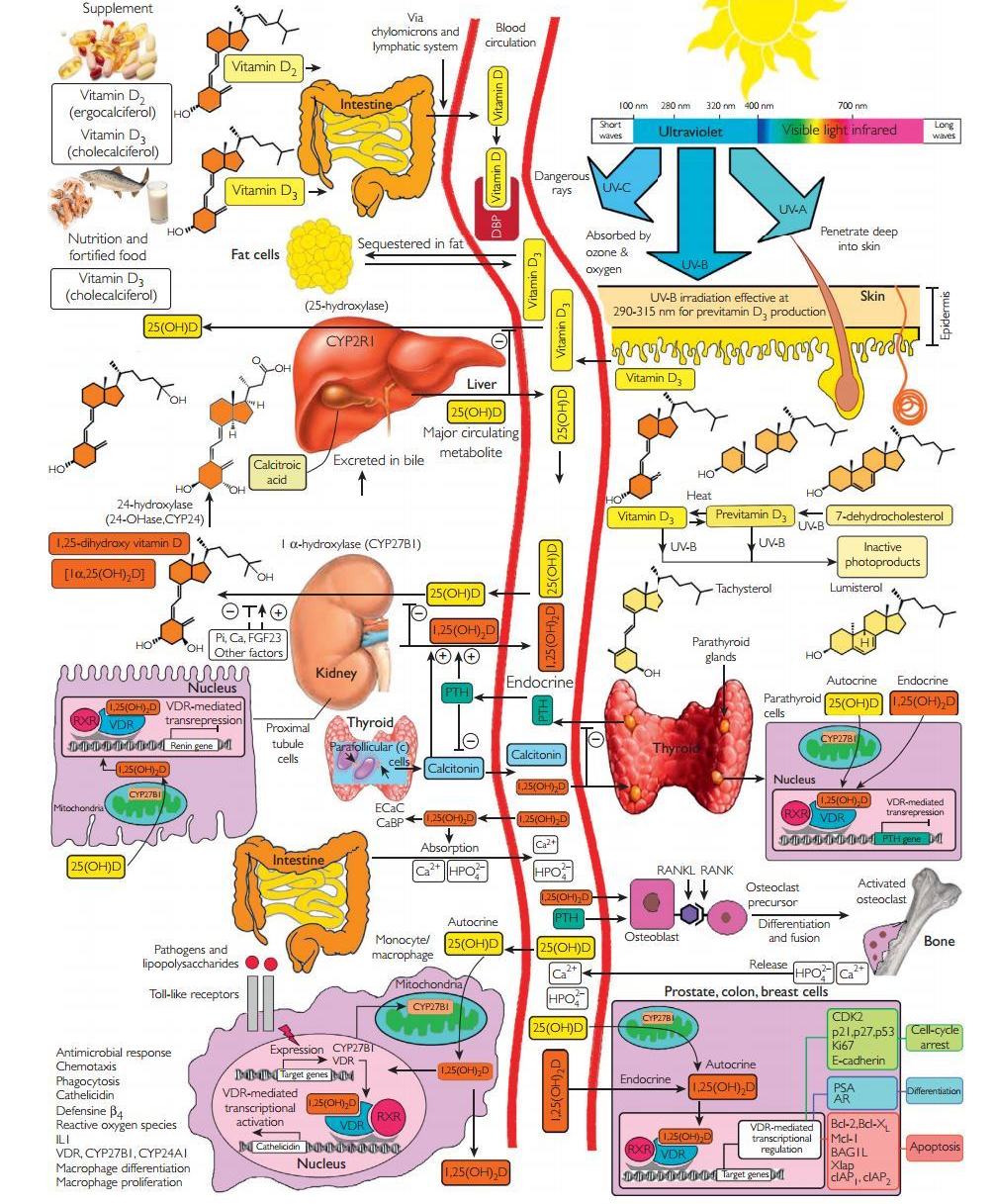
Schematic representation ofthe synthesis and metabolism of vitamin D for skeletal and nonskeletal function. 1 -OHase = 25-hydroxyvitamin D-1 a-hydroxylase; 24-OHase = 25-hydroxyvitamin D-24-hydroxylase; 25(OH)D = 25-hydroxyvitamin D; 1,25(OH)2D = 1,25-dihydroxyvitamin D; CaBP = calcium-binding protein; CYP27B1, Cytochrome P450-27B1; DBP = vitamin D—binding protein; ECaC = epithelial calcium channel; FGF-23 = fibroblast growth factor-23; PTH = parathyroid hormone; RANK = receptor activator ofthe NF-kB; RANKL = receptor activator ofthe NF-kB ligand; RXR = retinoic acid receptor; TLR2/1 = Toll-like receptor 2/1; VDR = vitamin D receptor; vitamin D = vitamin D2 or vitamin D3. Copyright Holick 2013, reproduced with permission.
One of the major physiologic functions of vitamin D is to maintain serum calcium and phosphorus levels in a healthy physiologic range to maintain a variety of metabolic functions, transcription regulation, and bone metabolism (Figure 1).2,7 The 1,25(OH)2D interacts with its VDR in the small intestine to increase the efficiency of intestinal calcium absorption from approximately 10% to 15% up to 30% to 40% and intestinal phosphorus absorption from approximately 60% to 80%.7 It also interacts with VDR in osteoblasts to stimulate a receptor activator of nuclear factor kB ligand, which, in turn, interacts with receptor activator of nuclear factor kBonimma-ture preosteoclasts, stimulating them to become mature bone-resorbing osteoclasts (Figure 1).7,18 The mature osteoclast removes calcium and phosphorus from the bone to maintain blood calcium and phosphorus levels. In the kidneys, 1,25(OH)2D stimulates calcium reabsorption from the glomerular filtrate.2,7
The VDR is present in most tissues and cells in the body.1,2,7,19-25 Many of these organs and cells, including the brain, vascular smooth muscle, prostate, breast, and macrophages, not only have a VDR but also have the capacity to produce 1,25(OH)2D.1,2,7,19-25 This production probably depends on the availability of circulating 25(OH)D, indicating the biological importance of sufficient blood levels of this vitamin D metabolite.2,15,26
The estimated 2000 genes that are directly or indirectly regulated by 1,25(OH)2D2,7,17-24,26 have a wide range of proven biological actions, including inhibiting cellular proliferation and inducing terminal differentiation, inhibiting angiogenesis, stimulating insulin production, inducing apoptosis, inhibiting renin production, and stimulating macrophage cathelicidin production.1,2,7,16,17,26 In addition, 1,25(OH)2D stimulates its own destruction in the kidneys and in cells that have a VDR and responds to 1,25(OH)2D by enhancing expression of the 25(OH)D—24-hydroxylase (CYP24A1) to metabolize 25(OH)D and 1,25(OH)2D into water-soluble inactive forms that are excreted in the bile (Figure 1).1,7,19,27
VITAMIN D METABOLISM DURING PREGNANCY
Vitamin D metabolism is enhanced during pregnancy and lactation. The placenta is formed at 4 weeks of gestation.2,25 From this time to term, 25(OH)D is transferred across the placenta, and the fetal cord blood concentration of 25(OH)D is correlated with the mother's concentration.27 However, the active metabolite 1,25(OH)2D does not readily cross the placenta.25,27 The fetal kidneys and the placenta provide the fetal circulation with 1,25(OH)2D by expressing CYP27B1 (Figure 2).28
The maternal (decidual) and fetal placental (trophoblastic) components of the placenta have CYP27B1 activity; cultured human syncytiotrophoblasts and decidual cells synthesize 1,25(OH)2D3.27 The spatiotemporal organization of placental CYP27B1 and the VDR across gestation has also been characterized, confirming that the enzyme and receptor are localized to the maternal and fetal parts of the placenta.29 Serum levels of DBP increase 46% to 103% during pregnancy, suggesting that DBP may play a role in directing vitamin D metabolism and function during pregnancy.2,27,30 The DBP has a much higher binding affinity for 25(OH)D than for 1,25(OH)2D, and in kidney epithelial cells, DBP plays a pivotal role in conserving 25(OH)D by facilitating the recovery of 25(OH)D from the glomerular filtrate.31,32
Transplacental transfer of calcium to the fetus is also facilitated by expression of all the key mediators of vitamin D metabolism in the placenta. Hormones involved in fetal growth and that influence CYP27B1 activity include insulin-like growth factor 1 and human placental lactogen, PTH-related protein (PTHrP), estra diol2,31,33,34 and prolactin.2,31,33,34 The PTHrP acts as a calciotropic hormone during fetal life and in lactation.35-37 The exact role of circulating PTHrP in pregnancy is unknown, but its rise may stimulate renal CYP27B1 and contribute to the increase in 1,25(OH)2D concentration and, indirectly, the suppression of PTH levels.27,35,37 The PTHrP arises from several sources, including the breast, myometrium, decidua, amnion, and fetal parathyroids.36 Several roles of PTHrP are postulated from animal studies, including fetal chondrocyte maturation, fetal calcium transfer, and stimulation of CYP27B1 activity.33,34,36
FIGURE 2.
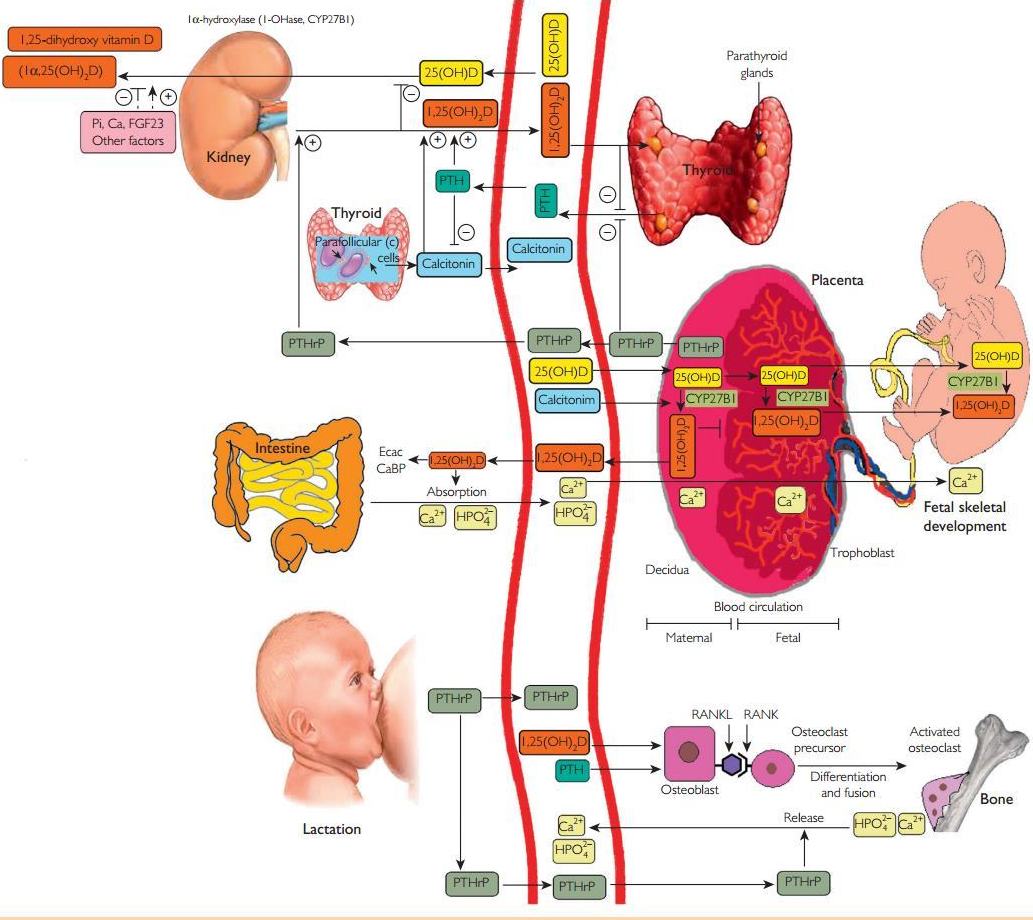
Vitamin D metabolism during pregnancy and lactation. Maternal 25(OH)D is thought to freely cross the human placenta. The placenta expresses vitamin D receptors (VDR) and also produces 1-OHase to convert 25(OH)D to 1,25(OH)2D. 1,25-dihydroxyvitamin D does not readily cross the placenta, and fetal1,25(OH)2D levels are normally lower than maternalserum levels. The low fetal concentrations of 1,25(OH)2Dreflect the low fetalPTH and high phosphorus concentrations, which suppress renal -OHase. Although PTHrP is elevated in the fetal circulation, it appears to be less able to stimulate the renal -OHase than PTH. Total (free and bound) ,25(OH)2D concentrations double or triple in the maternal circulation starting in the first trimester, but studies have only shown increased free concentrations during the third trimester. This increase is due to maternal synthesis by the renal -OHase. Vitamin D passes readily into breast milk, 25(OH)D passes very poorly,and ,25(OH)2D does not appear to pass at all.2 ,25(OH)2D levels fall rapidly after pregnancy and are normalduring lactation.7 Near-exclusive breastfeeding for 6 months leads, on average, to maternal calcium loss 4 times higher than that in pregnancy. Phosphorus can rise above the normal range, probably because of accelerated resorption from the skeleton. Parathyroid hormone-related protein levels are higher than PTH concentrations in nonpregnant women and show some pulsatility in response to suckling. Parathyroid hormone-related protein (produced by the lactating breast) in combination with low estradiol concentrations appears to drive the main physiologic adaptation to meet the calcium demands of lactation. Suckling and prolactin both inhibit ovarian function and stimulate PTHrP. Together, PTHrP and low estradiol concentrations stimulate skeletal resorption. Renal calcium reabsorption rates increase, presumably due to PTHrP, which mimics the actions of PTH on the renaltubules. For definitions of abbreviations, see Figure 1. Copyright Holick 2013, reproduced with permission.
Furthermore, the carboxy terminal of PTHrP (osteostatin) may suppress osteoclastic activity and may have a possible bone protection role in 32 35 37 the mother during pregnancy. ' - '
Calcitonin, an important component of calcium homeostasis during pregnancy,38'39 is known to promote transcription of CYP27B140 and may, therefore, be a key determinant of placental vitamin D metabolism.41 Thus, PTHrP and calcitonin, as well as other factors, cause 1,25(OH)2D levels to increase, being 2-fold higher in serum of women in the third trimester of pregnancy than in nonpregnant or postpartum women.2,27 Normally, 1,25(OH)2Dreg-ulates its own metabolism via a feedback loop such that elevated concentrations induce the expression of CYP24A1, with concomitant down-regulation of CYP27B1.7,25,42 This process results in a reduction of 25(OH)D and 1,25(OH)2Dlevels 9,29,30 However, during pregnancy, this process becomes uncoupled, resulting in elevated maternal concentrations of circulating 1,25(OH)2D.27,43 The placental methylation of the CYP24A1 promoter reduces the capacity for CYP24A1 induction and down-regulates basal promoter activity and abolishes vitamin D—mediated feedback activation. This epigenetic decoupling of vitamin D feedback catabolism also plays an important role in enhancing 1,25(OH)2D bioavailability at the fetomaternal interface.44
VITAMIN D, PLACENTA DEVELOPMENT, FETAL PROGRAMMING, AND EPIGENETIC MODIFICATION
Epidemiologic evidence has suggested a link between fetal life events and susceptibility to disease in adult life.45-47 This paradigm, referred to as fetal programming or developmental origins of health and disease, may have a profound effect on public health strategies for the prevention of major illnesses.2,48 The role of vitamin D in implantation tolerance and placental development has been studied. The 1,25(OH)2D3 regulates key target genes associated with implantation, such as Homeobox A10 (HOXA10), whereas the potent immunosuppressive effects of 1,25 (OH)2D3 suggest a role in placental develop-ment.49 Increasing expression of CYP27B1 and VDR in first-trimester human trophoblasts and deciduas50 may be related to the immunosuppressive effects of 1,25(OH)2D3 and may help improve implantation tolerance. Placental development plays a critical role in pregnancy health, and its link to maternal vitamin D deficiency may explain related adverse outcomes.5,45 In neonatal rats exposed prenatally to low maternal serum 25(OH)D levels, there was a general slowing of cardiac development, with significantly lower heart weights, decreased citrate synthase and 3-hydroxyacyl CoA dehydrogenase activity, and a 15% lower myofibrillar protein content.46 A 2-month-old human infant with dilated cardiomyopathy and severe vitamin D deficiency had dramatic improvement of her ejection fraction (17%-66%) after vitamin D supplementation.47 In addition, maternal vitamin D deficiency in rats stimulated nephrogenesis in offspring, with a 20% increase in nephron number but a decrease in renal corpuscle size observed between replete and deficient rats, despite there being no difference in body weight or kidney weight and volume.5,51 These findings support the role of vitamin D influencing fetal programming and placental development.
Epigenetic modification refers to heritable changes in gene expression that are not mediated by alterations in DNA sequence.52 This hypothesis, first articulated by Barker et al,53 postulated that in utero epigenetic fetal programming (as a result of environmental events during pregnancy) induced specific genes and genomic pathways that controlled fetal development and subsequent disease risk. The role of vitamin D in epigenetic modification and fetal programming could potentially explain why vitamin D has been reported to have such wide-ranging health benefits. Recent studies have suggested that epigenetic decoupling of vitamin D feedback catabolism plays an important role in maximizing 1,25(OH)2D bio-availability at the fetomaternal interface.25,44 Modified expression of the genes encoding placental calcium transporters, by epigenetic regulation by 1,25(OH)2D, might represent the means whereby maternal vitamin D status could influence bone mineral accrual in the neonate.54,55 Vitamin D deficiency during pregnancy may, therefore, not only impair maternal skeletal preservation and fetal skeletal formation but also influence fetal "imprinting" that may affect chronic disease susceptibility soon after birth as well as later in life (Figure 3).15,56 Trans-generational hormonal imprinting caused by vitamin D treatment of newborn rats has been previously reported.57 A recent study reported that VDR binds to the e germline gene promoter and exhibits transrepressive activity.58
FIGURE 3.
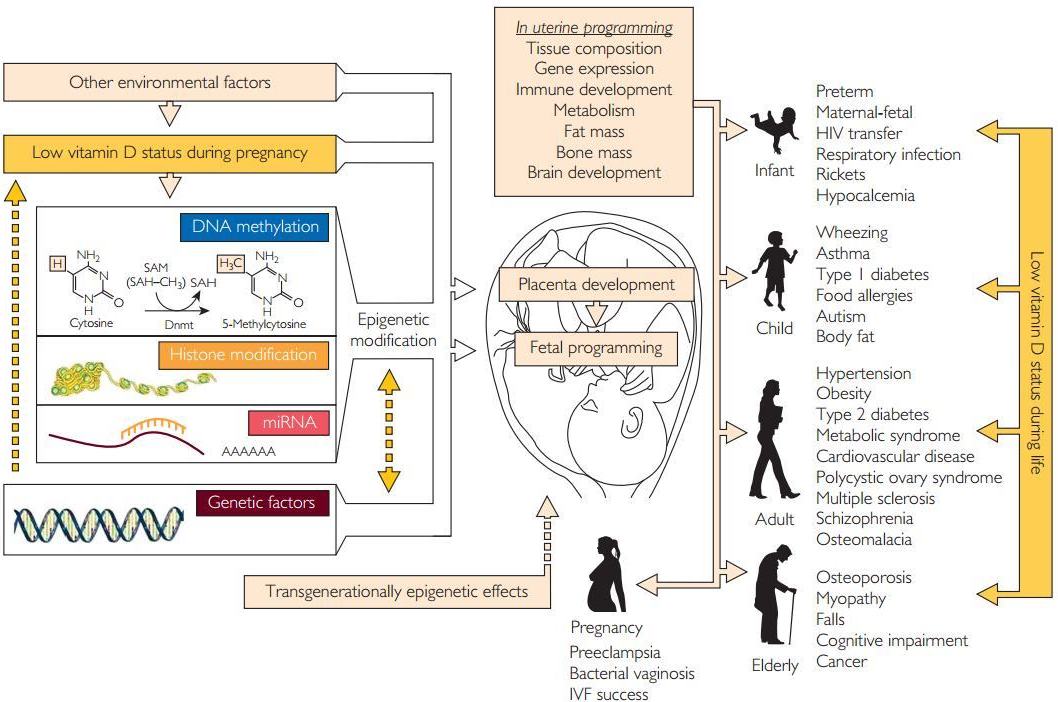
Vitamin D, placenta development, fetal programming, and epigenetic modification. A— adenosine; CH3 — methylgroup; HIV — human immunodeficiency virus; IVF — in vitro fertilization; miRNA, micro RNA; SAH — S-adenosylhomocysteine; SAM— single carbon from adenosylmethionine. Copyright Holick 2013, reproduced with permission.
Inhibition of IgE production by 1,25(OH)2D was mediated by its transrepressive activity through the VDR-corepressor complex, affecting chromatin compacting around the Ie region.58 Also, the associations of early-life sun exposure and germ-line variation in VDR and CYP24A1 with non-Hodgkin lymphoma risk was reported in a clinic-based case-control study.59
DEFINITION OF VITAMIN D DEFICIENCY
The blood level of 25(OH)D is the best method to determine vitamin D status. Although 1,25 (OH)2Disthebiologicallyactiveform,itpro-vides no information about vitamin D status because it is often normal or even elevated in children and adults who are vitamin D deficient.7,15,60-63 Recently, the Institute of Medicine (IOM) and the Endocrine Society released separate guidelines for vitamin D requirements.60,62 The recommended dietary allowances (RDAs) of the IOM and the Endocrine Society guidelines for vitamin D intake are summarized in Figure 4.
The revised guidelines by the IOM stress that the daily requirements for vitamin D are generally met by most of the population and are appropriate to reach the "sufficient" level of 20 ng/mL (to convert to nmol/L, multiply by 2.496).62 The IOM guidelines used a population model to prevent vitamin D deficiency in 97.5% of the general population. Also, note that the IOM report focuses only on bone health (calcium absorption, bone mineral density, and osteomalacia/rickets) and found no evidence that a serum 25(OH)D concentration greater than 20 ng/mL had beneficial effects at a population level. However, considering the available evidence on skeletal and extraskeletal effects of vitamin D, the few negative studies, and the lack of toxicity potential of vitamin D supplementation at
FIGURE 4.
Vitamin D intakes recommended by the Institute of Medicine and the Endocrine Practice Guidelines Committee. 25(OH) D — 25-hydroxyvitamin D; AI— adequate intake; RDA — recommended dietary allowance; SE — standard error; UL— tolerable upper intake level. Copyright Holick 2013, reproduced with permission.
recommended doses, the US Endocrine Society, which used a medical model, recommended that serum 25(OH)D levels of 30 ng/mL should be attained to avoid other risks connected with an inadequate vitamin D status.7,60 Therefore, the Endocrine Society recommended that vitamin D deficiency be defined as a 25(OH)D level of 20 ng/mL or less, vitamin D insufficiency as 21 to 29 ng/mL, and vitamin D sufficiency as 30 ng/mL or greater for children and adults.60 It suggested that maintenance of a 25(OH)D level of 40 to 60 ng/mL is ideal (this takes into account assay variability) and that up to 100 ng/mL is safe.60
MUSCULOSKELETAL CONSEQUENCES OF VITAMIN D DEFICIENCY
According to current evidence from biochemical testing, observational studies, and randomized controlled trials (RCTs), serum 25(OH)D levels of at least 20 ng/mL are required for normalization of PTH levels, to minimize the risk of osteomalacia, and for optimal bone and muscle function, with many experts regarding 30 ng/mL as the threshold for optimal bone health.7,16,61,64-66 The skeletal consequences of 25(OH)D insufficiency include secondary hyperparathyroidism, increased bone turnover and bone loss, and increased risk of low-trauma fractures.7,15,61,64
The most common etiology of rickets, historically and presently, is vitamin D deficiency. Low maternal 25(OH)D levels were found to correlate with increased fetal distal femoral splaying, determined by ultrasonography measurements of femoral length and metaphyseal width.63,65 Children begin to manifest classic clinical signs of rickets between 6 months and 1.5 years that include rachitic rosary, widened epiphyseal plates at the end of long bones, and bowing deformities of the legs.66 A common early symptom in newborns is excessive sweating due to neuromuscular irritability,66 and a 25(OH)D level less than 20 ng/mL is common in children presenting with vague limb or back pain.
From a skeletal perspective for adults, evidence from RCTs suggests that vitamin D may be considered a threshold nutrient, with little bone benefit observed at levels of 25(OH)D above which PTH is normalized.62,67 A literature review of 70 studies generally found a threshold for a decline in serum PTH levels with increasing serum 25(OH)D levels, but there was no consistency in the threshold level of serum 25(OH)D, which varied from 20 to 50 ng/mL.68 Astudy of 4100 older adults (>60years old) from the Third National Health and Nutrition Examination Survey (NHANES III) found that higher 25(OH)D levels were associated with better lower extremity function.61 Much of the improvement occurred at 25(OH)D levels ranging from 9 to 16 ng/mL but continued to be seen at levels up to 40 ng/mL.69 A systematic review revealed that supplemental vitamin D at daily doses of 800 to 1000 IU consistently had beneficial effects on muscle strength and balance.70 Several RCTs have reported positive effects of vitamin D supplementation on muscle function and fall prevention.71-73 Adequate calcium intake is imperative to gain optimal benefit from improving the vitamin D status in those with insufficient 25(OH)D levels.67 In contrast, a study of 173 young Asian Indian females revealed that after supplementation with vitamin D3 (60,000 IU/wk for 8 weeks followed by 60,000 IU every 2 weeks) and calcium (500 mg twice per day for 6 months), and despite significant improvement in serum 25(OH)D levels, there was no significant change in their skeletal muscle strength.74 Thus, age, baseline and final 25(OH)D concentrations, and whether and how much calcium supplementation was included in the clinical trial could affect outcome measures related to muscle performance and vitamin D status.
Proximal muscle weakness is a prominent clinical feature of vitamin D deficiency.7,60 The relative contributions of vitamin D and calcium for reducing fracture risk remain unclear75 because improving calcium intake is also associated with suppression of PTH levels independent of vitaminD status.67,76,77 A meta-analysis of data from RCTs found a dose-response relationship between a higher vitamin D dose and higher achieved serum 25(OH)D levels, with prevention of falls and fractures.73 The greatest benefit was observed at 700 to 1000 IU/d or a mean serum 25(OH)D concentration of 30 to 44 ng/mL.71,73 Similar results were reported in a more recent meta-analysis of pooled participant-level data from 11 double-blind RCTs of oral vitamin D supplementation, with or without calcium, compared with placebo or calcium alone in persons 65 years or older.78 Reduction in the risk of fracture occurred only at the highest vitamin D intake level (median, 800 IU/d; range, 792-2000 IU/d), with a 30% reduction in the risk of hip fracture and a 14% reduction in the risk of any nonvertebral fracture.78 This reduction was independent of the assigned treatment dose of vitamin D, age group, sex, type of dwelling, and study.78 Several previous meta-analyses have suggested that the dose of vitamin D is irrelevant when vitamin D is combined with calcium.79-82 In contrast, a pooled subgroup analysis of the 8 double-blind RCTs that used vitamin D combined with calcium indicated that with combined supplementation, the risk of fracture was reduced only at the highest actual intake level of vitamin D. These findings support that a 25(OH)D level of more than 24 ng/mL may be most beneficial for reducing the risk of fractures.78
With a similar tone and theme, a report from the US Preventive Services Task Force concluded that current evidence is insufficient to assess the balance of benefits and harms of combined vitamin D and calcium supplementation for the primary prevention of fractures in premenopausal women or in men.83 Furthermore, they concluded that there was insufficient evidence to assess the balance of benefits and harms of daily supplementation with greater than 400 IU of vitamin D3 and greater than 1000 mg of calcium for primary prevention of fractures in noninstitutionalized postmenopausal women.
They recommended against daily supplementation with 400 IU or less of vitamin D3 and 1000 mg or less of calcium for the primary prevention of fractures in noninstitutionalized post-menopausal women. They also stated that it was unclear whether higher doses of vitamin D and calcium are effective in preventing fractures in postmenopausal women, younger women, or men.83 The Task Force, however, concluded that vitamin D supplementation is effective in preventing falls in community-dwelling adults 65 years or older, which, in turn, reduces the risk of fracture. This could help explain the observation by the Women's Health Initiative (WHI) that, in the subgroup of long-adherent women who took their calcium and vitamin D, there was a reduced risk of hip but not total fractures.84 Therefore, what is still unknown is whether adequate intake of calcium, especially from dietary sources, and maintenance of serum 25(OH)D levels of at least 20 ng/mL as recommended by the IOM62 or at least 30 ng/mL as recommended by the Endocrine Society60 throughout life will reduce the risk of fracture. Most evidence suggests that adequate calcium and vitamin D intake along with exercise during childhood will maximize bone mineral content that can be sustained in young and middle-aged adults as long as they also have a healthy lifestyle, adequate calcium intake, and a healthy vitamin D status.60-62,84-86 Accruing maximum bone mineral content during childhood, and maintaining peak bone mineral density in young and middle-aged adults, will likely reduce the risk of fracture later in life, when there is a disruption in bone remodeling due to menopause and aging.
Recent recommendations of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO)87 for the optimal management of elderly and postmenopausal women regarding vitamin D supplementation have also indicated that patients with serum 25(OH)D levels less than 20 ng/mL have increased bone turnover, bone loss, and, possibly, mineralization defects compared with patients with serum 25(OH)D levels of 20 ng/mL or greater. Similar relationships have been reported for frailty, nonverte-bral and hip fracture, and all-cause mortality, with poorer outcomes at less than 20 ng/mL.87 Thus, ESCEO recommended that 20 ng/mL be the minimal serum 25(OH)D concentration at the population level and in patients with osteoporosis to ensure optimal bone health. Also, in fragile elderly individuals who are at elevated risk for falls and fractures, ESCEO recommended a minimal serum 25(OH)D level of 30 ng/ mL for the greatest effect on fracture.87 This coincides with the recommendation from the Endocrine Society60 and with the observation of Priemel et al,79 who reported that of 675 presumed healthy adults (aged 20-90+ years) who died in an accident, 36% had evidence of osteomalacia. However, Priemel et al79 observed no osteomalacia in those who had a 25(OH)D level greater than 30 ng/mL.
EVIDENCE-BASED SKELETAL AND NONSKELETAL HEALTH BENEFITS OF VITAMIN D
Observational studies have found a decreased risk of many disorders, including certain types of cancer, mental disorders, infectious disease, cardiovascular disease, type 2 diabetes mellitus, and autoimmune disorders, associated with serum 25(OH)D levels greater than 28 to 32 ng/mL.7,60,67 It has, therefore, been argued that 25(OH)D levels should be in the range of 28 to 40 ng/mL to maximize these nonskeletal benefits.1,2,7,19,60,61
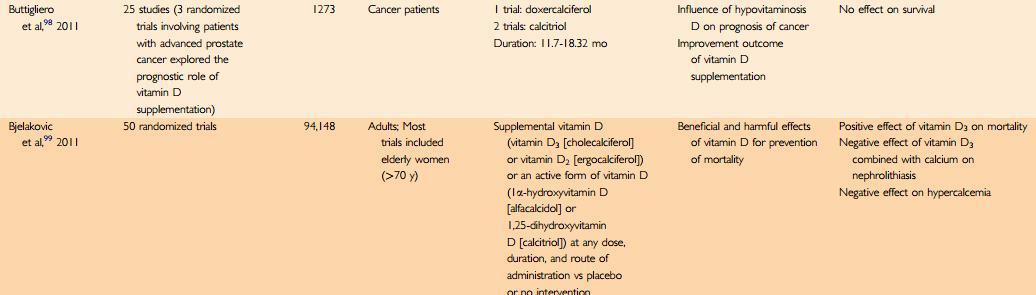
The results of some clinical trials provide evidence confirming the results of observational and association studies, whereas others do not. The Table summarizes the meta-analyses on vitamin D supplementation, comparing the beneficial and nonbeneficial effects of vitamin D supplementation in randomized trials for musculoskeletal and nonskeletal outcomes. The Table provides the foundation for clinical decision making for recommending vitamin D supplementation and identifies gaps in our knowledge that require additional RCTs to provide insights as to whether vitamin D supplementation has nonskeletal health benefits.
TABLE. Summary of Meta-analyses of Vitamin D Supplementation


See also in Vitamin D Life Overview Meta-analysis of Vitamin D
VITAMIN D AND NONSKELETAL HEALTH ASSOCIATIONS AND MECHANISMS
Cancers
Association studies have related higher serum levels of 25(OH)D to reduced incidence of many types of cancers. It has been hypothesized that the local conversion of 25(OH)D to 1,25(OH)2D in healthy cells in the colon, breast, and prostate can help prevent malignancy by inducing cellular maturation, inducing apoptosis, and inhibiting angiogenesis while enhancing the expression of genes including P21 and P27 to control cellular proliferation (Figure 1).1,2,7,16,26 Another vitamin D— regulated gene is CYP3A4, whose protein product detoxifies the bile acid lithocholic acid.114 Lithocholic acid is believed to damage the DNA of intestinal cells, and it may promote colon carcinogenesis. Stimulating the production of a detoxifying enzyme by 1,25(OH)2D could explain a protective role for improving vitamin D status against colon cancer.114 Because vitamin D regulates a gamut of physiologic processes, including immune modulation, resistance to oxidative stress, and modulation of other hormones, it is not surprising that low vitamin D status has been associated with increased risk of several cancers and cancer mortality.7,61,115-126 As the importance of non-coding RNAs has emerged, the ability of 1,25(OH)2D to regulate microRNAs (miRNAs) has been found in several cancer cell lines, patient tissues, and sera. In vitamin D3 intervention trials, significant differences in miRNAs were observed between treatment groups or between baseline and follow-up.116 In patient sera from population studies, specific miRNA differences were associated with serum levels of 25(OH)D. The findings thus far indicate that increasing vitamin D3 intake in patients and 1,25(OH)2D3 in vitro not only regulates specific miRNA(s) but also up-regulates global miRNA levels.116
Epidemiologic studies have suggested that adequate levels of 25(OH)D are critical for the prevention of various solid tumors, including prostate, breast, ovarian, and colon cancers.97,114,115,117-120 A meta-analysis for the US Preventive Services Task Force regarding vitamin D supplementation concluded that each 4-ng/mL increase in blood 25(OH)D levels was associated with a 6% reduced risk of colo-rectal cancer but not with statistically significant dose-response relationships for prostate and breast cancer.97 In a large prospective study of lethal prostate cancer (1260 cases vs 1331 controls), men with the highest quartile of plasma 25(OH)D levels had less than half the risk of lethal prostate cancer compared with men with the lowest quartile of plasma 25(OH)D levels.115 A meta-analysis including 1822 colon and 868 rectal cancers reported an inverse association between circulating 25(OH)D levels and colorectal cancer, with a stronger association for rectal cancer.97,121 Participants in the WHI who had a baseline 25(OH)D level less than 12 ng/mL and who took 400 IU of vitamin D3 and 1000 mg of calcium daily had a 253% increased risk of colorectal cancer compared with women who took the same amount of vitamin D3 and calcium for 7 years and had baseline serum 25(OH)D levels greater than 24 ng/mL.84,122
Although cross-sectional data have many limitations, the findings are hypothesis generating and can be used to develop protocols for RCTs.84,123,124 The findings from prospective case-control cohort studies in which blood collection occurred many years before diagnosis add another dimension to the evidence.118 The results of these studies generally support vitamin D supplementation in those with "low" vitamin D status. However, some have argued for caution before increasing 25(OH)D levels and associated dosing regimens beyond quantities clearly supported by RCTs and meta-analyses.7,97,103 There are now several observational studies reporting a U- or J-shaped association between some cancers and serum 25(OH)D and latitude or UV-B radiation levels, in which those in the highest percentiles have an inverse risk compared with those in the lowest.118,125-127 Many RCTs that were evaluated for nonskeletal benefits of vitamin D had problems with a high incidence of nonadherence, misinterpretation of the original data, and use of doses of vitamin D below the 2010 IOM recommendations.62,123,124,128 A good example is the WHI.129 More than 50% of participants in the WHI admitted not taking their calcium and vitamin D daily, and blood concentrations of 25(OH)D were often not measured at baseline or at study end.124,129 Furthermore, the authors acknowledged that the 400 IU of vitamin D was inadequate to raise the blood level of 25(OH)D above 30 ng/mL, which most studies have suggested is required to reduce cancer risk and other nonskeletal acute and chronic diseases.7,26,61,127,128 A reanalysis of the WHI concluded that in 15,646 women (43%) who were not taking personal calcium or vitamin D supplements at randomization, the calcium and vitamin D intervention significantly decreased the risk of total, breast, and invasive breast cancers by 14% to 20% and the risk of colorectal cancer by 17%. In another RCT, a 60% reduction in all cancers was observed in postmenopausal women who ingested 1100 IU of vitamin D3 and 1500 mg of elemental calcium daily for 4 years.130 There is conflicting evidence about vitamin D's relationship with risk of pancreatic cancer. A study of more than 120,000 men and women from the Health Professionals Follow-up Study and the Nurses' Health Study found that participants with higher dietary intake of vitamin D had a progressively lower risk of pancreatic cancer compared with those who had the lowest intake.131 In a study of men and women enrolled in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial,132 no association between serum 25(OH)D levels and pancreatic cancer risk was observed. A pooled analysis of 5 nested case-control studies reported an inverse association between plasma levels of 25(OH)D and the subsequent risk of pancreatic cancer.133 Compared with individuals with 25(OH)D levels less than 20 ng/mL, those with 25(OH)D levels of 20 ng/mL or greater experienced an approximately 30% lower risk of pancreatic cancer.
Grant120,134,135 reported that more than 13 cancers were reduced by adequate exposure to solar UV-B radiation. He calculated that in a span of 24 years (1970-1994), 566,400 Americans died of cancer because of inadequate exposure to solar UV-B radiation.120,134-136 He also estimated that 50,000 to 63,000 Americans and 19,000 to 25,000 British citizens in the United Kingdom die prematurely of cancer each year due to vitamin D deficiency.135,136 A large collaborative effort analyzed data from 10 prospective cohort studies to examine whether serum 25(OH)D levels were associated with 7 rare cancers.137 The National Cancer Institute Cohort Consortium Vitamin D Pooling Project of Rarer Cancers included information on serum 25(OH)D levels and the incidence of rare cancers in a subset of more than 12,000 men and women. The researchers matched participants on date and season of blood collection and used other statistical techniques to adjust for seasonal variation in serum 25(OH)D levels. When the data from the different studies were pooled, there was no overall association between vitamin D status and risk of non-Hodgkin lymphoma or cancers of the endometrium, esophagus, stomach, kidney, or ovary. In contrast, a recent review of ecological studies associating solar UV-B exposure—vitamin D and cancers found strong inverse correlations with solar UV-B irradiance for 15 types of neoplasms: bladder, breast, cervical, colon, endometrial, esophageal, gastric, lung, ovarian, pancreatic, rectal, renal, and vulvar cancers and Hodgkin and non-Hodgkin lymphoma.138 Weaker evidence was observed for 9 other types of cancer: brain, gallbladder, laryngeal, oral/pharyngeal, prostate, and thyroid cancers; leukemia; melanoma; and myeloma.138 Although there was compelling evidence for the association between vitamin D intake and cancer risk, a meta-analysis by Buttigliero et al98 found no effect of vitamin D supplementation on survival in patients with cancer.
Mortality
Vitamin D deficiency is associated with an increased risk of total mortality.139 Most, but not all, studies documented increased mortality rates in patients with low 25(OH)D concentrations. In a study of 24 ,5 4 individuals from the primary care sector, a reverse J-shaped relation was reported between serum level of 25(OH)D and all-cause mortality, with the lowest mortality rate at 20 to 24 ng/mL.126 This finding underscores the importance of not only including the very low (4 ng/mL) but also the higher (56 ng/mL) levels of 25(OH)D in the analysis.126 It also raises several questions. How do patients who had a 25(OH)D level greater than 50 ng/mL attain such a high level, which is usually observed only in Africans living outdoors?128,140 These people are likely taking megadoses of vitamin D and possibly other supplements or are being treated for vitamin D deficiency. In some instances, studies are misrepresented or misinterpreted. For example, the IOM reported in their overview that there was evidence of increased mortality for those with a 25(OH)D level greater than 30 ng/mL. However, one of the studies used to support this IOM conclusion actually stated that mortality rates were reduced until the blood level of 25(OH)D reached 50 ng/mL and that mortality rates possibly increased only in women who had 25(OH)D levels greater than 50 ng/mL.141 When these J curves are plotted, we are not informed what percentage of study participants had a 25(OH)D level greater than 50 ng/mL. By some estimates, less than 10% of patients have a 25(OH)D level greater than 50 ng/mL, and in a recent meta-analysis,126 only 1.5% of participants had a 25(OH)D level greater than 50 ng/mL. This raises questions about the validity of the so-called J-U curve analyses.
A meta-analysis of prospective cohort studies including 5562 deaths of 62,548 participants suggested a nonlinear decrease in mortality risk as circulating 25(OH)D concentration increases, with optimal outcomes occurring at concentrations of approximately 30 to 35 ng/ mL.142 In a similar meta-analysis, vitamin D intake and blood 25(OH)D levels were inversely associated with risk of colorectal cancer, and a 10-ng/mL increase in blood 25(OH)D levels conferred a risk rate (RR) of 0.74.143 A meta-analysis of prospective studies of 6853 patients with chronic kidney disease found that the mortality risk decreased by 14% per 10-ng/mL increase in 25(OH)D levels.144 The major cause of mortality was cardiovascular disease.
In a recent meta-analysis with 70,528 randomized participants (86.8% females) with a median age of 70 years, vitamin D supplementation with or without calcium reduced mortality by 7%. However, vitamin D supplementation alone did not affect mortality, but risk of death was reduced if vitamin D was given with calcium.145 The Ludwigshafen Risk and Cardiovascular Health Study is a cohort study of patients referred for coronary angiography between 1997 and 2000, from which 1801 with the metabolic syndrome were investigated. Mortality was tracked for a median of 7.7 years.146 Multivariable survival analysis was used to estimate the association between serum 25(OH)D levels and mortality. After full adjustment, including the metabolic syndrome components, patients with optimal 25(OH)D levels had a substantial reduction in all-cause (hazard ratio [HR], 0.25; 95% CI, 0.13-0.46) and cardiovascular disease (HR, 0.33; 95% CI, 0.16-0.66) mortality rates compared with those with severe vitamin D deficiency. For specific cardiovascular disease mortality, there was a strong reduction in sudden death (HR, 0.15; 95% CI, 0.040.63) and congestive heart failure (HR, 0.24; 95% CI, 0.06-1.04) but not for myocardial infarction. The reduction in the mortality rate was dose dependent for each of these causes.146 Consistent with the beneficial effect of vitamin D on risk of mortality, a meta-analysis of 50 randomized trials by Bjelakovic et al found a positive effect of vitamin D3 on mortality.
Cardiovascular Disorders and Type 2 Diabetes Mellitus
Observational studies in humans found that 25(OH)D and 1,25(OH)2D levels are inversely related to coronary artery calcifications147,148 and are lower in patients with myocardial infarc-tion.14 An in vitro study suggested that low 25(OH)D levels influence the activity/expression of macrophages and lymphocytes in atherosclerotic plaques, thus promoting chronic inflammation in the artery wall.150 Additionally, 1,25(OH)2D3 inhibited foam cell formation and promoted angiogenesis in endothelial colony-forming cells in vitro, possibly due to an increase in vascular endothelial growth factor expression and pro—matrix metalloproteinase-2 activity.4,151 A short course of treatment with vitamin D (4000IU for 5 days) effectively attenuated the increase in circulating levels of inflammatory cytokines after an acute coronary event.150 These findings provide support for the antiinflammatory effects of vitamin D on the vascular system and suggest mechanisms that mediate some of its cardioprotective properties.4,150 In addition, low 25(OH)D concentrations result in elevations in PTH levels, which have been linked to insulin resistance and significant increases in the serum levels of many acute phase proteins.14
Wang et al152 studied 173 Framingham Offspring Study participants (mean age, 59 years; 55% women; all of white race) without previous cardiovascular disease. During mean follow-up of 5.4 years, 120 individuals experienced a first cardiovascular event. Individuals with 25(OH) D levels less than 15 ng/mL had a multivariable-adjusted HR of 1.62 for incident cardiovascular events compared with those with 25(OH)D levels of 15 ng/mL or greater. This effect was evident in participants with hypertension (HR, 2.13; 95% CI, 1.30-3.48) but not in those without hypertension.152 Observational studies indicated that a serum 25(OH)D level less than 30 ng/mL was strongly associated with hypertension and metabolic syndrome.153 This effect is thought to be partly mediated through regulation of the renin-angiotensin-aldosterone axis.154 The Intermountain Heart Collaborative Study Group prospectively analyzed a large electronic medical records database that contained 41,504 patient records. Serum 25(OH)D levels less than 30 ng/mL were associated with highly significant increases in the prevalence of diabetes, hypertension, hyperlipidemia, and peripheral vascular disease. Serum 25(OH)D levels were also highly associated with coronary artery disease, myocardial infarction, heart failure, and stroke and with incident death, heart failure, coronary artery disease/ myocardial infarction, stroke, and their composite.153 Black normotensive children who received 2000 IU/d of vitamin D3 were compared with those who received 400 IU/d for 16 weeks in an RCT. Teenagers who received 400 IU/d of vitamin D3 increased their mean ± SD plasma levels of 25(OH)D from 13.6±4.2 to 23.9±7.2 ng/mL and had no reduction in arterial wall stiffness. In contrast, teenagers who received 2000 IU/d of vitamin D3 increased their mean ± SD plasma levels of 25(OH)D from 13.2±3.4 to 34.2± 12.1 ng/mL and significantly lowered their arterial wall stiffness.155 This finding is supported by the observation that serum 25(OH)D levels less than 30 ng/mL were strongly associated with hypertension, elevated blood glucose, and metabolic syndrome in adolescents.156 Children with vitamin Ddeficiency or insufficiency had a 2.5-fold higher risk of an elevated blood glucose level, a 2.4-fold increased risk of elevated blood pressure, and a 4-fold increased risk of metabolic syndrome, a prelude to type 2 diabetes.156
A meta-analysis of 11 prospective studies involving 3612 cases and 55,713 noncase participants provided the largest and most comprehensive assessment thus far of the association between circulating 25(OH)D levels and type 2 diabetes. It suggested a strong inverse association between serum 25(OH)D concentration and incidence of type 2 diabetes. The combined RR of 0.59 suggested that the risk of future diabetes may be reduced by 41% (95% CI, 33%-48%)by having a serum 25(OH)D level greater than 32 ng/mL compared with a serum 25(OH)D level less than 19.5 ng/mL at baseline.157 The MID-SPAN family study was a prospective study of 1040 men and 1298 women from the West of Scotland recruited in 1996 and followed up for a median of 14.4 years.158 Plasma levels of 25(OH)D less than 15 ng/mL were not associated with a risk of cardiovascular disorders in this cohort with very low 25(OH)D levels. The median plasma 25(OH)D level was 18.6 ng/mL, and the median vitamin D intake was 3.2 mg/d (128 IU/d). However, there was some evidence that a 25(OH)D level less than 15 ng/mL was associated with all-cause mortality.158 There was an association between 25(OH)D levels and incidence of type 2 diabetes, but there was no evidence in this study of a beneficial effect of vitamin D supplementation on type 2 diabetes outcomes.106 A meta-analysis of 15 trials by George et al106 did not find sufficient evidence to recommend vitamin D supplementation for improving glycemia or insulin resistance in patients with diabetes, normal fasting glucose levels, or impaired glucose tolerance. Similarly, Wang et al109 and Pittas et al110 concluded in their meta-analyses that evidence from limited data suggested that vitamin D supplements at moderate to high doses may reduce the risk of cardiovascular disease,109 but most studies that used lower doses found no clinically meaningful effect.110
Autoimmune Diseases
Vitamin D has been defined as a natural immune modulator. Epidemiologic, genetic, and basic science studies indicate a potential role of vitamin D in the pathogenesis of certain systemic and organ-specific autoimmune diseases, such as type 1 diabetes mellitus, MS, rheumatoid arthritis (RA), and Crohn disease (CD).159 Vitamin D'seffects on the innate immune system are predominantly through the toll-like receptors and on the adaptive immune system through T-cell differentiation, particularly the T helper cell (TH)type 17 response. Because TH17 cells are critical in the pathogenesis of RA, this has led to an interest in the effects of vitamin D deficiency in RA.160 Vitamin D inhibits immune reactions in general, but it enhances the transcription of endogenous antibiotics, such as cathelicidin and defensins.26,161 Vitamin D suppresses autoimmune disease pathology by regulating the differentiation and activity of CD4+ T cells, resulting in a more balanced Th1/Th2 response that favors less development of self-reactive T cells and autoimmunity.162 The TH1-dependent autoimmune diseases, including MS, type 1 diabetes, CD, and RA, are also inhibited by 1,25(OH)2D3 owing to inhibition of antigen presentation, reduced polarization of Th0 cells to Th1 cells, and reduced production of cytokines from the latter cells.161 The 1,25(OH)2D3 down-regulated the proinflammatory cytokine (interleukin 1b,interleukin 6, and tumor necrosis factor) production in human activated macrophages by significantly decreasing the aromatase activity, especially in the presence of an estrogenic milieu, such as in RA synovial tissue.163 A prospective cohort study of 29,368 women aged 55 to 69 years without a history of RA found an inverse association between vitamin D intake and RA after 11 years of followup.164 Therewas a34% reduction in the development of RA with greater vitamin D intake. Women using a multivitamin with 400 IU of vitamin D reduced their risk of RA by 40%.164 Use of a high-dose vitamin D3 analogue resulted in improvement of symptoms of RA in 89% of patients, with 45% of patients entertaining a complete remission.165 Recent evidence has suggested a significant inverse relationship between serum 25(OH)D levels and visual analog scale scores in patients with RA.166 Very low serum 25(OH)D levels (<6 ng/mL) were characterized by patients being positive for rheumatoid factor, a high percentage of patients with very high disease activity, and a high percentage of patients requiring treatment with at least 3 disease-modifying antirheumatic drugs.167
There is a large body of evidence linking a lack of vitamin D early in life to the development of type 1 diabetes.168 Vitamin D supplementation during infancy was reported to confer partial protection against b-cell autoimmunity.169 There is consistent evidence from observational studies for potential long-term programming effects of vitamin D supplementation on immunologic diseases, such as type 1 diabetes, MS, asthma, and allergic diseases.5 There was a 63% decreased risk of islet cell antibodies in offspring with a single standard deviation (156 IU) increase in recalled maternal dietary vitamin D intake during pregnancy.5 Similarly, higher maternal cod liver oil (a source of vitamin D) intake during pregnancy was associated with a decreased risk of type 1 diabetes in offspring, and fetal exposure to vitamin D deficiency was linked to a higher metabolic and cardiovascular disease risk in adult life.170
A Finnish study (10,366 children) found that children who regularly took the recommended dose of vitamin D (2000 IU/d) had a rate ratio of 0.22 (95% CI, 0.05-0.89) compared with those who regularly received less than the recommended amount.171 The 1,25(OH)2D3 has been reported in animal models and in cultured cells to improve insulin production, modulate T- and b-cell activity, enhance phagocytic killing activity, improve vascular smooth muscle resistance, and reduce the risk of autoimmune diseases.7'155'162 In contrast, in healthy youth (aged 8-18 years), plasma 25(OH)D concentrations had no independent relationship with parameters of glucose ho-meostasis and in vivo insulin sensitivity and b-cell function relative to insulin sensitivity.172 It remains to be determined whether in youth with dysglycemia the relationships are different and whether vitamin D optimization enhances insulin sensitivity and b-cell function.172
Evidence continues to accumulate supporting a protective role for vitamin D in MS risk and progression. Notable recent findings are that high 25(OH)D levels at the time of a first demyelinating event predicts a lower MS risk and a decreased risk of MS in offspring whose mothers had high 25(OH)D levels.173 An American study of more than 187,000 women followed up for 10 to 20 years reported promising results with women taking at least 400 IU of supplemental vitamin D daily. The risk of MS was decreased by 41%.174 An epigenetic study in lymphoblastoid cell lines reported relevant insights into how vitamin D may influence the immune system and the risk of MS through VDR interactions with the chromatin state inside MS-associated genomic regions.175 Higher 25(OH)D levels were associated with decreased exacerbation risk in relapsing-remitting MS.175 However, the literature is limited by small study sizes, heterogeneity of dosing, form of vitamin D tested, and clinical outcome measures.176 Whether vitamin D3 immunomodulatory effects can be translated into clinical benefits in patients with MS is still a matter of debate.176 High doses of vitamin D3 (up to 280,000 IU/ wk for 6 weeks) have been used safely in patients with MS.177,178 Blood levels of 25(OH) D rose to a mean of 154 ng/mL without causing hypercalcemia. The progression and activity of MS were not affected in this study, but the number of gadolinium-enhancing lesions per patient assessed by nuclear magnetic brain scan was significantly reduced.177 A trial using high-dose vitamin D2 to achieve 25(OH)D levels of 52 to 78 ng/mL did not reduce magnetic resonance imaging lesions in relapsing-remitting MS.178 In a trial using escalating doses up to 40,000 IU/d of vitamin D3 for 28 weeks followed by 10,000 IU/d for 12 weeks, there were no significant adverse events, and there seemed to be significantly less progression of disability in the treatment group.179
A chromatin immunoprecipitation sequencing—defined genome-wide map of VDR binding reported that there were 2776 "binding sites" on the human genome with at least 229 genes associated with type 1 diabetes and CD.180 In a clinical trial in patients with CD in remission, 1200 IU of vitamin D3 daily increased mean ± SD serum 25(OH)D levels from 27.6±12.4 to 38.4±10.8 ng/mL after 3 months.181 The relapse rate was numerically lower in patients treated with vitamin D3 (6 of 46 or 13%) than in patients treated with placebo (14 of 48 or 29%), although this did not quite reach significance (P=.06). Monocyte-derived dendritic cells (DCs) from 20 patients with CD were cultured with either 25(OH)D3 or 1,25(OH)2D3 and were matured with lipopoly-saccharide (LPS).182 After stimulation with 25(OH)D3, DCs from patients with CD displayed a reduced response to LPS with a diminished capability to activate T cells compared with DCs stimulated with LPS alone. Compared with LPS alone, both metabolites of vitamin D3 reduced the ability of DCs to activate lymphocytes. These data indicate that intrinsic activation of 25(OH)D3 to 1,25(OH)2D3 occurs in DCs from patients with CD and provides evidence that higher serum 25(OH)D3 levels can potentially modulate DC function in CD.182 Although several studies reported the immuno-modulatory effects of vitamin D on biological functions and developing processes of autoimmune diseases, there is no strong evidence for recommending vitamin D supplementation to prevent or manage the autoimmune diseases on the basis of the results of some short-term clinical trials.177,178,181
Respiratory Tract Diseases and Wheezing Disorders
At the turn of the past century, children with rickets were at higher risk for upper respiratory tract infections and for dying of them.26,183 Macrophages have a VDR, and when they ingest an infectious agent, such as tuberculosis bacillus, the toll-like receptors are activated, resulting in signal transduction to increase the expression of VDR and CYP27B1.7'26'28 In turn, 25(OH)D is converted to 1,25(OH)2D, which signals the nucleus to increase the expression of cathelicidin, a defensin protein that kills infective agents, such as tuberculosis bacillus.7,26,28
Cord blood 25(OH)D levels were associated with tolerogenic immune regulation and fewer respiratory tract infections in newborns.184 Also, high 25(OH)D levels during maternity were associated with a decrease in childhood wheezing by nearly 50% compared with low maternal 25(OH)D levels. Newborns with 25(OH)D levels less than 10 ng/mL were twice as likely to develop respiratory tract infections compared with those with levels of 30 ng/mL or greater, and every 4-ng/mL increase in the cord blood 25(OH)D level lowered the cumulative risk of wheezing by age 5 years.184 Serum concentrations of 25(OH)D in 198 healthy adults revealed that a concentration of 38 ng/ mL or higher reduced the risk of acute viral respiratory tract infections and number of days ill by 2-fold.185 Japanese children who received 1200 IU/d of vitamin D from December through March compared with those who received placebo reduced their risk of influenza A by 42%.186 It was also observed that children who took vitamin D daily had a relative risk reduction of 93% for having an asthma attack compared with children who did not take a vitamin D supplement.186 Vitamin D has also been implicated in the reversal of corticosteroid resistance and in airway remodeling, which are the hallmarks of chronic obstructive pulmonary disease and severe asthma. Dietary vitamin D may regulate epigenetic events, in particular on genes that are responsible for chronic obstructive pulmonary disease susceptibility.187
The potential role of vitamin D in reducing the risk of allergies also may be related to epigenetic regulation.188,189 Misdirected epigenetic programming offered an explanation for why vitamin D deficiency in pregnancy may be associated with increased allergy rates in the offspring. The cord blood level of 25(OH)D found a U-shaped association, with a 2.4-fold odds ratio (OR) of low and a 4-fold OR of high levels of 25(OH)D to develop allergen-specific IgE.188,190 Eczema was significantly more likely in those with 25(OH)D levels less than 20 ng/mL compared with those with 25(OH)D levels of 30 ng/mL or greater (OR, 2.66; 95% CI, 1.24-5.72; P=.01).189 On a molecular level, maternal vitamin D intake during pregnancy increased the messenger RNA levels of immunoglobulin-like transcript (ILT) 3 and ILT4 in umbilical cord blood.191 Because ILT3 and ILT4 are critical for the generation of T suppressor cells and the induction of immunologic tolerance, this finding may point toward an early induction of tolerogenic immune responses by maternal vitamin D intake in the developing child. In addition, vitamin D stimulates natural killer cells that are known to play an immunoregulatory role in the prevention of autoimmune diseases.2 Thus, although vitamin D can favorably influence several pathways associated with respiratory tract diseases, there are few clinical trials to support the beneficial effect of vitamin D supplementation for these patients. Meta-analyses on respiratory outcomes111 and recovery from tuberculosis112 did not report a beneficial effect of supplementation for patients with cystic fibrosis or tuberculosis, respectively.
Neurologic Disorders
The brain has a VDR and has the ability to produce 1,25(OH)2D3. In vivo mouse studies found that in utero hypovitaminosis D impairs brain development and leads to persistent changes in the adult brain.192 The 1,25(OH)2D3 is rapidly incorporated into embryonic hippocampal cells, moves into the nucleus, and then returns to the cytoplasm.193 These events delay cell proliferation and induce cell differentiation characterized by the expression of differentiation markers, modification of soma lengthening, and increase in neurite length and branching.193 At birth, rats with prenatal vitamin D deficiency had heavier and longer brains, enlarged lateral ventricles, and decreased cortical thickness.5,192,194-196 Evidence from human studies is scanty. One recent study found that higher maternal serum 25(OH)D levels in late pregnancy (<12 vs >30 ng/mL) were associated with larger head circumference of offspring at 9 years old but not with measures of cognition or psychological health.5,194 In addition, there may be a critical window during late gestation in which vitamin D insufficiency precipitates an altered adult behavioral phenotype.195 In rats, offspring of vitamin D—deficient mothers had significant impairment of latent inhibition (ability to ignore irrelevant stimuli), a feature often associated with schizophrenia, whereas those transiently depleted had subtle and discrete alterations in learning and memory.196 In a Finnish birth cohort study, 9114 individuals were drawn from the northern Finland 1966 birth cohort.197 In males, the use of at least 2000 IU of vitamin D during the first year of life was associated with a reduced risk of schizophrenia (RR, 0.23; 95% CI, 0.06-0.95) compared with those taking lower doses.197
There is minimal evidence for an association of low maternal vitamin D status with risk of autism.5 Children of dark-skinned mothers, particularly immigrants to locations with low ambient UV radiation, such as Minnesota, may be at increased risk, but this finding has been inconsistent.198
The 1,25(OH)2D3 seems to have a neuro-protective role, inducing remyelination by endogenous progenitor cells and stimulation of amyloid-P clearance by macrophages of patients with Alzheimer disease.199 A vitamin D3—enriched diet correlated with a decrease in the number of amyloid plaques and inflammation in the brains of APPP mice.199 These observations suggest that a vitamin D3—enriched diet may reduce the risk of Alzheimer disease as well as depression and neurocognitive disorders. An Australian study of 743 white pregnant women found that maternal vitamin D insufficiency during pregnancy is significantly associated with offspring language impairment.200 Vitamin D deficiency was also associated with prominent changes in behavior and brain neurochemistry in the adult mouse.201 In the follow-up of a British birth cohort (n=7401), current and subsequent risk of depression in middle adulthood was associated with low serum 25(OH)D levels.202 This study provides support for a lower risk of depression with serum 25(OH)D levels between 20 and 34 ng/mL. A meta-analysis of cohort studies reported that there was a significantly increased HR of depression for the lowest vs highest vitamin D categories (HR, 2.21; 95% CI, 1.40-3.49). 203 In a community setting, depressed adults had significantly lower 25(OH)D levels than those without depression.204 A variety of studies found an association between a low level of 25(OH)D and a high depression score.205,206 Patients who received 400 to 800 IU of vitamin D with calcium for 6 to 12 months did not have an improvement in their mental health scores. However, patients who received 400 to 800 IU of vitamin D for 5 days with calcium or a single 100,000-IU dose of vitamin D had an improvement in the assessments of depression.207,208 Although there is a strong association between risk of neurologic disorders and serum 25(OH)D concentrations, there are only a few short-term clinical trials of vitamin D in patients with MS that have not reported benefit and no clinical trials evaluating other neurologic disorders.177,178
Adverse Pregnancy Outcomes
A recent meta-analysis of data from 24 studies found that women with circulating 25(OH)D levels less than 20 ng/mL in pregnancy experienced an increased risk of preeclampsia (OR, 2.09; 95% CI, 1.50-2.90), gestational diabetes mellitus (OR, 1.38; 95% CI, 1.12-1.70), preterm birth (OR, 1.58; 95% CI, 1.08-2.31), and small-for-gestational-age (OR, 1.52; 95% CI, 1.08-2.15).209 However, many of these outcomes are rare and require a large sample size to study, representing a challenge for cohorts with a limited number of preserved samples. Experimental studies have provided evidence of disrupted vitamin D metabolic homeostasis in the preeclamptic placenta and have suggested that increased oxidative stress could be a causative factor of altered vitamin D metabolism in preeclamptic placentas.50 In normal placenta, DBP, CYP24A1, and VDR expressions were localized mainly in trophoblasts, whereas CYP2R1 and CYP27B1 expressions were localized mainly in villous core fetal vessel endothelium.50 Protein expression of CYP2R1 and VDR were reduced, but CYP27B1 and CYP24A1 expressions were elevated in preeclamptic compared with nor-motensive placentas.50 A similar pattern was observed in an invitro model that found that hypoxia induced down-regulation of DBP, CYP2R1, and VDR and up-regulation of CYP27B1 and CYP24A1 50 These data indicate that fetal (trophoblastic) autocrine synthesis of 1,25(OH)2D3 may play a pivotal role in controlling placental inflammation and preeclampsia.
One of the main pathogenic features of preeclampsia is maternal endothelial dysfunction that results from impaired angiogenesis and reduced endothelial repair capacity. The 1,25(OH)2D3 improves the angiogenic properties of endothelial progenitor cells. These findings could explain the positive influence of vitamin D3 in reducing preeclampsia risk.151
There was an inverse association with having a cesarean delivery and serum 25(OH)D levels. In a case-control study, after adjustment for race, age, educational level, insurance status, and alcohol use, women with 25(OH)D levels less than 15 ng/mL were almost 4 times as likely to have a cesarean delivery than were women with 25(OH)D levels of at least 15 ng/mL.210
A meta-analysis of 3 trials involving 463 women suggested that women who received vitamin D supplements during pregnancy less frequently had a baby with a birth weight less than 2500 g than did those who received no treatment or placebo; the statistical significance was borderline.89 In terms of other conditions, there were no significant differences in adverse effects, including nephrotic syndrome, stillbirths, and neonatal deaths, between women who received vitamin D supplements and women who received no treatment or pla-cebo.89 A meta-analysis indicated a significant inverse relation between serum 25(OH)D level and the incidence of gestational diabetes mellitus. Overall, vitamin D deficiency (25[OH]D <20 ng/mL) in pregnancy was significantly related to the incidence of gestational diabetes mellitus, with an OR of 1.61.211 However, it remains unclear whether this association is causal owing to the observational design of the studies. Recently, meta-analyses by Thorne-Lyman and Fawzi88 and De-Regil et al89 reported a similar beneficial effect of vitamin D supplementation on birth weight but no significant effect on other maternal and neonatal outcomes.
ASSESSING VITAMIN D STATUS
Although the generally accepted measure of vitamin D status is circulating 25(OH)D concentration, there is little consensus on which assay method should be used. Commonly used assays include competitive protein-binding assay, radio-immunoassay, enzyme immunoassay, chemiluminescence immunoassay, high-performance liquid chromatography, and liquid chromatography—tandem mass spectrometry (LC-MS/MS), each with its own advantages and disadvantages.212,213 Binkley et al214 reported that 25 (OH)D results differed widely depending on the laboratory and the method used, with the mean result (from 10 healthy adults) varying from 17.1 to 35.6 ng/mL. A study conducted by the Vitamin D External Quality Assessment Scheme found a 31% overestimation by one immuno-assay method.215 Its specificity needs to exclude significant interferences from the C-3 epimer of 25(OH)D, which is more prevalent in infants younger than 1 year.216
DiaSorin radioimmunoassays (DiaSorin Corp) used in the NHANES III had a mean bias of greater than 12% comparing the vitamin D status of the US population of 1988-1994 with that of 2000-2004. This difference was probably caused by changes in reagents and calibration lots performed by the manufacturer.217,218 This makes diagnostic and therapeutic decisions on the basis of absolute cutoff values for vitamin D deficiency extremely prob-lematic219,220 and hinders the comparability of results from prospective and epidemiologic studies. Since November 2010, efforts have been made to recalibrate 25(OH)D measurements from all NHANES samples with LC-MS/MS. This effort is within the context of an international approach to standardization of 25(OH)D measurements in national surveys, the Vitamin D Standardization Program, and publication of the results is planned for the middleof20 1 3.221 To ensure that laboratories are providing accurate testing results, it is important that their vitamin D testing method measures total 25(OH)D levels [25(OH)D2 and 25(OH)D3] and has acceptable precision. The immunoassay remains the predominant mode of measurement for 25(OH)D. Most, if not all, of these assays have problems with equi-molarrecoveryofthe 25(OH)D2 and 25(OH)D3 levels.222 The level of 25(OH)D2 is underestimated by 20% to 80% and can vary for different patients who received vitamin D2 in the same assay. Standardization of all assays has been improved but not resolved with the currently available reference materials, as evidenced by the Vitamin D External Quality Assessment Scheme.222 The choice of method for each laboratory remains a balance mainly among turnaround time, convenience, cost, and the specificity and accuracy of the information obtained.208 Recognizing the importance of a 25(OH)D2 and 25(OH)D3 reference material, the National Institute of Standards and Technology released a 4-level Standard Reference Material set, SRM972.221 Treatment with vitamin D2, therefore, may not be accurately monitored using many of the commercial assays because these antibody assays often underestimate 25(OH)D2 levels and, thus, total 25(OH)D levels, which is what they record in the report. This issue is most important in patients who experience no improvement with replacement therapy with vitamin D2 (the most commonly used Food and Drug Administration—approved pharmaceutical form of vitamin D); the absence of a rise in the total 25(OH)D level may indicate nonadherence or malabsorption.223 For these patients, use of the gold standard LC-MS/MS would quantitatively report 25(OH)D2, 25(OH)D3, and total 25(OH)D levels.
VITAMIN D STATUS DURING PREGNANCY, BIRTH, AND CHILDHOOD
Maternal vitamin D deficiency predisposes to low vitamin D stores in the newborn and increases infantile rickets224 because the mother is the only source of vitamin D during pregnancy. The prevalence of vitamin D deficiency and insufficiency during pregnancy is of special concern and ranges from 8% to 100%, depending on the country of residence and the definitions of vitamin D deficiency and insufficiency (Figure 5).2 In the United States, vitamin D deficiency and insufficiency is estimated to be 27% to 91% in pregnant women.2 As shown in Figure 5, this rate is estimated to be 36% to 65% in Canada, 45% to 98% in Asia, 70% to 100% in Europe, and 25% to 65% in Australia and New Zealand.124,128
The prevalence of vitamin D deficiency and insufficiency in children in China is high, especially in children aged 6 to 16 years.211 In the United States, it is estimated that 50% of children aged 1 to 5 years and 70% of children aged 6 to 11 years are vitamin D deficient or insufficient.156 Recent studies reported that adolescents and young adults are also at risk for vitamin D deficiency.16,128,217 Also, a high prevalence of vitamin D deficiency was reported in a cross-sectional study conducted at a tertiary care center in western India.225
Evidence suggests that children and adults in the United States are becoming more vitamin D deficient and insufficient because of an increase in the incidence of obesity, a decrease in milk consumption, and an increase in sun protection. 15,217
This recent evidence emphasizes the high prevalence of vitamin D deficiency throughout the world, not only in at-risk groups (Figure 5).7,15,217,224-230
PREVALENCE OF VITAMIN D DEFICIENCY IN ADOLESCENTS AND ADULTS
It has been estimated that 20% to 80% of US, Canadian, and European men and women are vitamin D deficient.228,229 The prevalence of serum 25(OH)D levels less than 20 ng/mL was almost one-third of the US population (32%).217 More than 70% of non-Hispanic black individuals and more than 40% of Hispanic/Mexican individuals were at risk for a 25(OH)D level less than 20 ng/mL.228 In a national Canadian cohort, serum 25(OH)D levels less than 30 ng/mL were evident in 57.5% of men and in 60.7% of women, and they rose to 73.5% in spring (men) and 77.5% in winter (women).229 In the Healthy Lifestyle in Europe by Nutrition in Adolescence study, 25(OH)D levels less than 30 ng/mL were reported to be approximately 80% in adolescents from the 9 European countries.230 Levels of 25(OH)D were higher in northern Europe than in southern Europe and were higher in western Europe than in eastern Europe.230 The higher levels in northern Europe were also observed in some multicenter studies in which a single laboratory facility was used.230
The higher serum 25(OH)D levels in Norway and Sweden are probably due to a high intake of fatty fish and cod liver oil. The lower serum 25(OH)D levels in Spain, Italy, and Greece may be due to more skin pigmentation, sunshine-avoiding behavior, and air pollution with ozone and nitrogen dioxide, which reduce sun-induced vitamin D production.226
In the Middle East and Asia, vitamin D deficiency in children and adults is highly prevalent.7,227 Children and adults of color are especially at high risk owing to the inefficient cutaneous production of vitamin D31,2,7 In a study on the vitamin D status of Australian adults, vitamin D deficiency (25[OH]D <20 ng/mL) was 31% (22% in men and 39% in women); 73% had 25(OH)D levels less than 30 ng/mL.226 Women who practice purdah (ie, the use of clothing and other approaches to screen themselves from men and strangers) and children and adults who avoid all sun exposure or wear sunscreen protection are equally at high risk.7,231
CAUSES OF VITAMIN D DEFICIENCY AND RISK FACTORS
Traditional risk groups for vitamin D deficiency include pregnant women, children, older persons, the institutionalized, and non-Western immigrants.7,228 The major source of vitamin D for children and adults is exposure to natural sunlight.7,61
FIGURE 5.
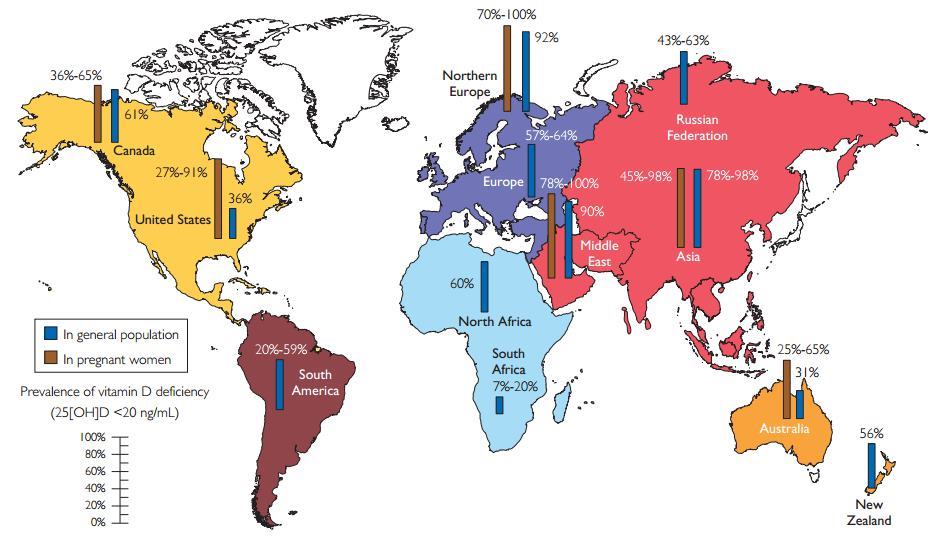
Reported incidence of vitamin D deficiency defined as a 25-hydroxyvitamin D (25[OH]D) levelbelow 20 ng/mL around the globe in pregnant women and the generalpopulation. To convert 25(OH)D values to nmol/L, multiply by 2.496. Copyright Holick 2013, reproduced with permission.
See also in Vitamin D Life Overview Pregnancy and vitamin D
The Maasai and Hadzabe tribes in Tanzania (East Africa) with traditional lifestyles, living in the presumed cradle of humankind, who are exposed daily to tropical sunlight had a mean circulating 25(OH)D level of 46 ng/mL.140
See also in Vitamin D Life Chart of Vitamin D levels vs race - April 2013
A variety of factors influence the cutaneous production of vitamin D. A sunscreen with a sun protection factor of 30 applied properly reduces the ability of the skin to produce vitamin D by as much as 95% to 99%. People of color who have natural sunscreen protection from their increased melanin pigment are less efficient by more than 90% in producing vitamin D in their skin compared with white individuals.232 In addition, air pollution with increased ozone and nitrogen dioxide levels (both known to compromise several health outcomes) absorbs UV-B radiation and is an often-neglected risk factor for hypovitaminosis D.61,233 Important risk factors for vitamin D deficiency are shown in Figure 6.
The prevalence of vitamin D deficiency and insufficiency is affected by seasonal variation and latitude. The prevalence increases in late winter/spring and decreases in summer.234 A study of the effect of education on vitamin D status found that low-educated women had lower 25(OH)D levels compared with high-educated women, and women in the lowest 25(OH)D quartile had a higher risk of small-for-gestational-age offspring.235
The elderly population is particularly at risk for clinical complications related to low 25(OH) D levels. With increasing age, solar exposure is usually limited because of changes in lifestyle factors, such as clothing and less outdoor activity. Diet may also become less varied, with a lower natural vitamin D content. Most important, however, the cutaneous production of vitamin D after exposure to solar UV-B radiation decreases with age because of atrophic skin changes, with a reduced amount of its precursor 7-DHC.236,237 A comparison of the amount of previtamin D3 produced in skin from 8- to 18-year-old individuals with the amount produced in skin from 77-to 82-year-old individuals revealed that aging can decrease by greater than 2-fold the capacity of the skin to produce previtamin D3.237
FIGURE 6.
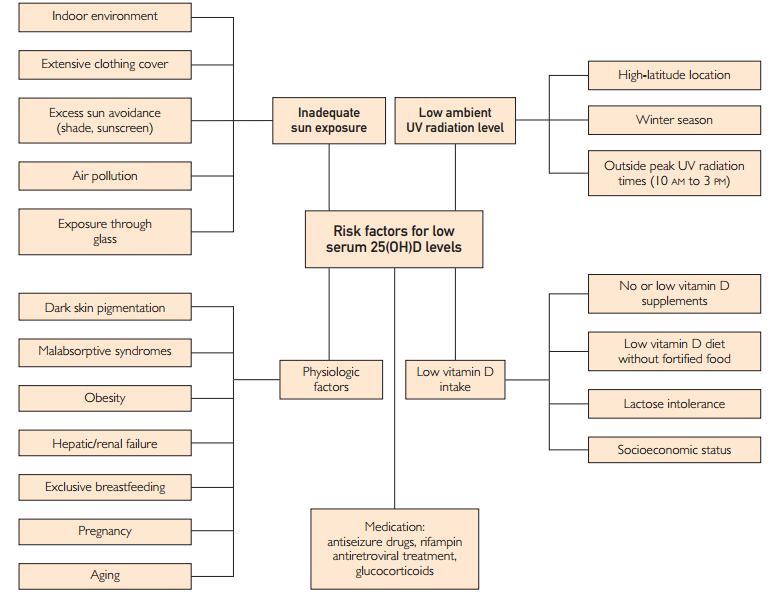
Risk factors for low vitamin D status. 25(OH)D — 25-hydroxyvitamin D. Copyright Holick 2013, reproduced with permission.
See also in Vitamin D Life Risk Factors for Vitamin D Deficiency
Although the heritability of vitamin D status seems considerable, the specificgenetic determinants of 25(OH)D levels are only beginning to be identified. A recent examination of 141 single nucleotide polymorphisms (SNPs) in a discovery cohort of 1514 white participants from the community-based Cardiovascular Health Study found that lower serum 25(OH)D levels were associated with HRs for the risk of the composite outcome of 1.40 for those who had 1 minor allele at rs7968585 (in VDR) and 1.82 for those with 2 minor alleles.238,239 This candidate gene study indicates that known associations of low serum 25(OH)D levels with clinical outcomes may vary according to genetic differences in the VDR. In black patients, there were significant associations in 3 SNPs in vitamin D pathway genes (rs2282679, rs2298849, and rs10877012), all of which replicate earlier findings in populations of European ancestry.239 Included among these was rs2282679, a highly significant result from 2 recent genome-wide association studies (GWASs),240,241 one of which reported a 49% increased risk of vitamin D deficiency (25[OH]D <20 ng/mL) associated with the rs2282679 minor allele in white individuals.241 Another study of genetic predictors of 25(OH)D in black individuals involved 513 participants from 42 families in Los Angeles, California, and evaluated 30 SNPs in DBP, VDR, and CYP27B1.242 Recent epigenomic findings confirmed 3 genes (DHCR7, CYP2R1, and CYP24A1) of the 4 genes in the GWAS findings, which reinforces the crucial roles played by those 3 genes in vitamin D metabolism.243 DHCR7 encodes the enzyme 7-DHC reductase, which converts 7-DHC to cholesterol, thereby removing the substrate from the synthetic pathway of vitamin D3239 DHCR7 is a novel gene for association with 25(OH)D levels, as identified in 2 recent GWASs.240,241 CYP24A1, which encodes 25(OH)D—24-hydroxylase, has been identified as a candidate gene for vitamin D insufficiency in one GWAS but not in the other.240-242 This mitochondrial protein initiates the degradation of 1,25(OH)2D3 and plays a role in calcium homeostasis and vitamin D metabolism. These epigenomic findings suggest that individuals with vitamin D deficiency are more likely to have reduced synthesis and increased catabolism of 25(OH)D and 1,25(OH)2D.243
The genetic contributions to circulating 25(OH)D represent a complex trait for which family studies have estimated heritability ranging from 43% to 80%.244 Genomic and epigenomic data integration provided greater understanding of the physiology and etiology of the complex traits. Further elucidation of the genetic architecture of this complex trait beyond environmental determinants of 25(OH)D has the potential to identify those at risk for vitamin D insufficiency.244 It may also provide a useful proxy for lifetime vitamin D exposure that may be applied in instrumental variable analyses investigating the association between vitamin D and common complex diseases. However, a recent GWAS of prospec-tively collected 25(OH)D data in 5 studies with 5575 individuals reported that known GWAS-associated SNPs explain only a fraction of the observed variance in circulating 25(OH)D levels (ie, approximately 5.2%)244 On rare occasions, some patients who deny taking a vitamin D supplement have unexplained high normal 25(OH)D levels in the range of 40 to 80 ng/mL. It is believed that this is due to a genetic mutation of the cyp24A1 that reduces the catabolism of 25(OH)D and 1,25(OH)2D and can be a cause of infantile hypercalcemia.245 Therefore, these recent genomic and epigenetic data provide additional evidence of genetic-environmental interactions and their effects on circulating 25(OH)D levels.
TREATMENT AND PREVENTION OF VITAMIN D DEFICIENCY AND INSUFFICIENCY WITH SUN EXPOSURE AND UV-B IRRADIATION
Humans obtain a considerable amount of their vitamin D requirement from sun exposure.7,140 Although excessive exposure to sunlight increases the risk of nonmelanoma skin cancer, which is easy to detect and easy to treat, there is no evidence that sensible sun exposure, as our hunter-gatherer forefathers likely experienced, increases risk.124,246 More importantly, the most deadly form of melanoma skin cancer that occurs on the least sun-exposed areas is less likely to occur in adults who have outdoor occupations.1,124,246,247 Therefore, it is not unreasonable to consider sensible sun exposure as a good source of vitamin D.7,124 An adult in a bathing suit exposed to 1 minimal erythemal dose (slight pinkness to the skin 24 hours after exposure) is the equivalent to taking approximately 20,000 IU (500 mg) of vitamin D2 orally.7,15 Thus, exposure of arms and legs to 0.5 minimal erythemal dose is equivalent to ingesting approximately 3000 IU of vitamin D3.7,60 Adults who frequented a tanning salon had robust levels of 25(OH)D, on average 46 ng/mL, and had higher bone mineral density in their hips compared with healthy adults who did not go to a tanning salon in Boston, Massachusetts, at the end of winter.248 It was estimated that if all the people in the United States were to double their solar UV-B irradiance to raise their serum 25(OH)D levels to 45 ng/mL, the net result could be as many as 400,000 reduced deaths compared with only 11,000 increased deaths from melanoma and other skin cancer.249 Time of day during sun exposure, season, latitude, and degree of skin pigmentation dictate how much vitamin D3 is produced during sun exposure. Exposure of the arms and legs (abdomen and back when possible) to sunlight 2 to 3 times a week for approximately 25% to 50% of the time it would take to develop a mild sunburn (minimal erythemal dose) will cause the skin to produce enough vitamin D. For a white person, if 30 minutes of June noontime sun would cause a mild sunburn, then 10 to 15 minutes of exposure followed by good sun protection should be sufficient to produce adequate vitamin D.7 There is no need to ever expose the face because although it is the most sun exposed of all the body areas, it provides little vitamin D3 A free app, dminder.info, provides the user with information about sensible sun exposure and vitamin D production. For patients with fat malabsorption syndromes that render oral consumption of supplemental vitamin D ineffective, exposure to a lamp that emits UV-B radiation can be effective in raising blood levels of 25(OH)D.250
Food Sources
Very few foods naturally contain vitamin D; examples of foods with ample vitamin D stores include wild-caught salmon and UV-exposed mushrooms.7 Foods fortified with vitamin D usually contain 100 IU per serving. An analysis of the vitamin D intake of children and adults in the United States revealed that they were unable to achieve the RDA for vitamin D from any dietary sources.251
Vitamin D intake can be increased by eating foods fortified with vitamin D. A recent systematic review found that food fortification with vitamin D (especially in milk) is effective in significantly increasing 25(OH)D levels in the population.7,252 Other foods include some cereals, juices, other dairy products, and some margarines. A mean individual intake of approximately 11 mg/d (440 IU/d) from fortified foods (range, 120-1000 IU/d) increased 25(OH)D concentrations by 7.7 ng/mL, corresponding to a 0.48-ng/mL increase in 25(OH) D for each 40 IU (1 mg) ingested.252
Vitamin D Supplementation
The RDA for vitamin D and tolerable upper-limit levels vary in different age groups and in certain circumstances.7,60,62 Although it is recommended that RDAs of 600 to 800 IU daily should meet the requirements to optimize bone health62 in most of the population, higher vitamin D intakes (1000-2000 IU) are needed to reach and maintain 25(OH)D levels greater than 30 ng/mL.7,60 It is recognized that for every 100 IU of vitamin D ingested, the blood level of 25(OH)D increases by approximately 0.6 to 1 ng/mL.253 When the serum 25(OH)D level is less than 15 ng/mL, 100 IU of vitamin D will increase the 25(OH)D level by as much as 2 to 3 ng/mL.7,71 An effective strategy to treat vitamin Ddeficiency and insufficiency in children and adults is to give them 50,000 IU of vitamin D2 once a week for 6 and 8 weeks, respectively.60,254 To prevent recurrence of vitamin D deficiency in children, administration of 600 to 1000 IU/d is effective.60 For adults, to prevent recurrence of vitamin D deficiency, administration of 50,000 IU of vitamin D2 every 2 weeks is effective.7,60,255 This strategy was shown to be effective in maintaining blood levels of 25(OH)D at approximately 40 to 60 ng/mL for up to 6 years without any evidence of toxic effects.255
Vitamin D can be administered daily, weekly, monthly, or every 4 months to sustain an adequate serum 25(OH)D concentration.7,256-258 A bolus of high doses of vitamin D (up to 300,000 IU) can be initially used in persons with extreme vitamin D deficiency. Repeated boluses of high-dose vitamin D at 6- to 12-month intervals have been used in a nursing home setting, but a steady-state serum 25(OH)D concentration is likely to be maintained by more frequent, lower doses of vitamin D. One study has suggested that a 500,000-IU bolus dose of vitamin D3 increases the risk of fracture within 3 months,256 but other studies have reported reduced risk of fracture.257,258
Vitamin D Supplementation During Pregnancy and Lactation
The 25(OH)D passes from the placenta into the bloodstream of the fetus. Because the half-life for 25(OH)D is approximately 2 to 3 weeks, the infant can remain vitamin D sufficient for several weeks after birth, as long as the mother is vitamin D sufficient.2
In a study of 40 mostly black pregnant women who were documented to be ingesting approximately 600 IU of vitamin D a day, at the time that they gave birth,76% were vitamin D deficient as defined by the IOM cutoff value of a 25(OH)D level less than 20 ng/mL.259 Eighty-one percent of their newborns were vitamin D deficient.259 Maternal supplementation with 2000 and 4000 IU/d of vitamin D during pregnancy improved the maternal/neonatal vitamin D status.260 None of the pregnant women developed significant changes in their serum calcium or 24-hour urinary calcium levels. Evidence of risk reduction in infection, preterm labor, and preterm birth was suggestive, requiring additional studies powered for these end points.260,261
Human breast milk and unfortified cow's milk have little vitamin d.7,260,261 Only after lactating women were given 4000 to 6000 IU/d of vitamin D was enough vitamin D transferred in breast milk to satisfy the infant's requirement.260,261
Vitamin D Supplementation in Special Conditions
Because body fat can sequester vitamin D, it is now recognized that children and adults who are obese require 2 to 5 times more vitamin D to treat and prevent vitamin D deficiency.7,60 Patients taking antiseizure medications, AIDS medications, and glucocorticoids often require more vitamin D to satisfy their requirements.7,60 However, patients with granulomatous disorders, such as sarcoidosis and tuberculosis, are at risk for hypercalciuria and hypercalcemia when blood levels of 25(OH)D are greater than 30 ng/mL owing to the increased serum levels of 1,25(OH)2D produced in the macrophages in the granulomas.7 Therefore, their vitamin D intake needs to be carefully monitored and controlled.7,60 Hence, daily requirements of vitamin D to reach and maintain the desired serum 25(OH)D level can be estimated from the baseline 25(OH)D concentration. Supplemental vitamin D is preferentially administered orally or intramuscularly (not available in the United States), and the vitamin D—producing Sperti lamp can be used, where available, in patients with malabsorption syndromes.250,262
Type of Vitamin D Supplementation
Either vitamin D2 or vitamin D3 can be used for vitamin D supplementation, although there is controversy regarding vitamin D3 vs vitamin D2 for achieving and maintaining higher serum 25(OH)D levels. Although a recent meta-analysis indicated that vitamin D3 is more efficacious at raising serum 25(OH)D concentrations than is vitamin D2,2,102 several prospective studies have found them to be equally effective in raising and maintaining serum 25(OH)D levels in children and adults.263,264 Holick et al264 found that an 11-week course of treatment with 1000 IU/d of vitamin D2, 1000 IU/ d of vitamin D3, or a combination of 500 IU of vitamin D2 and 500 IU of vitamin D3 daily caused an equivalent increase in serum total 25(OH)D levels. Furthermore, the group that received vitamin D2 did not experience a significant change in serum 25(OH)D3 levels. Gordon et al265 and Thacher et al266 also found that in infants and toddlers treated for 6 weeks, 2000 IU of vitamin D2 and 2000 IU of vitamin D3 daily or a single dose of 50,000 IU of vitamin D2 or vitamin D3 were equally effective in increasing the serum total 25(OH)D level. The bioavailability of vitamin D3 is well established, and the bioavailability of vitamin D2 from mushrooms in humans has been found to be comparable with that of a vitamin D2 supplement.267 Finally, adults treated with vitamin D2 not only raised their total blood levels of 25(OH)D but also maintained total blood levels of 1,25(OH)2D to the same degree as adults who received the same dose of vitamin D3.263
SAFETY AND INTOXICATION
Vitamin D intoxication is characterized by hypercalcemia, hypercalciuria, and hyperphosphatemia, which, in turn, are responsible for soft-tissue and vascular calcifications and nephrolithiasis in the long term. Serum 25(OH)D levels are usually markedly elevated (>150 ng/ mL) in individuals with vitamin D intoxication.7,60,90 Daily doses of vitamin D3 up to 10,000 IU were safe in healthy males, and there was no evidence of hypercalcemia or hypercalciuria for 5 months.253,268 This amount is far above the tolerable upper level indicated in the IOM guidelines (4000 IU). Higher doses of vitamin D (up to 40,000 IU/d) are still safe provided that a serum 25(OH)D concentration of 200 ng/mL is not exceeded. A recent report of an infant inadvertently receiving 12,000 IU of vitamin D3 daily for 20 days and achieving a serum 25(OH)D level of 425 ng/mL had no signs of vitamin D intoxication. Once the vitamin D use was stopped, the serum 25(OH)D level was less than 100 ng/mL within 2 months.269
CONCLUSION
Vitamin D deficiency is a common underdiagnosed condition that has received increasing attention in the world. The US Endocrine Society guidelines and the IOM recommend screening only in populations at risk, as no evidence currently exists to support screening at a population level. Candidates for vitamin D screening include those who are at specific risk for vitamin Ddeficiency and patients who are experiencing or are at risk for specific medical conditions associated with hypovitaminosis D.
Recent evidence from hundreds of studies has suggested that vitamin D is important for reducing the risk of a variety of chronic illnesses. The identification of a VDR in most tissues and cells and the observation that a multitude of genes may be directly or indirectly regulated by 1,25(OH)2D have provided a rationale for the nonskeletal health benefits of vitamin D. A study in healthy adults who received either 400 or 2000 IU/d of vitamin D3 for 3 months in winter reported that 291 genes were either up-regulated or down-regulated. That these genes affected as many as 80 different metabolic pathways (from immune modulation to enhanced antioxidant activity) emphasizes the importance of improving the world's vitamin D status.17 The observation that 1,25(OH)2D may also influence epigenetics provides additional support for the concept that there is no downside to increasing the vitamin D status of children and adults. Vitamin Ddeficiency during pregnancy may adversely influence placental development and fetal programming. Vitamin D deficiency in both parents may influence adverse pregnancy outcomes and susceptibility to developing disease in adult life and even into the next generation.
There is potentially a great upside (in terms of improving overall health and well-being) to increasing serum 25(OH)D levels above 30 ng/mL. An effective strategy to prevent vitamin Ddeficiency and insufficiency is to obtain some sensible sun exposure, ingest foods that contain vitamin D, and take a vitamin D supplement.
Abbreviations and Acronyms:
CD = Crohn disease; DBP = vitamin D binding protein; DC = dendritic cell; ESCEO = European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis; GWAS = genome-wide association study; HR= hazard ratio; ILT = immuno-globulin-like transcript; IOM = Institute of Medicine; IVF = in vitro fertilization; LC-MS/MS = liquid chromatography— tandem mass spectrometry; LPS = lipopolysaccharide; miRNA = microRNA; MS = multiple sclerosis; NHANES = National Health and Nutrition Examination Survey; OR = odds ratio; PTH = parathyroid hormone; PTHrP = parathyroid hormone—related protein; RA = rheumatoid arthritis; RDA = recommended dietary allowance; RCT = randomized controlled trial; RR = risk rate; SE = standard error; SNP = single nucleotide polymorphism; TH = T helper cell; VDR = vitamin D receptor; WHI = Women's Health Initiative; 1,25(OH)2D= 1 a,25-dihydroxyvitamin D; 7-DHC = 7-dehydrocholesterol; 25(OH)D = 25-hydroxyvitamin D
Grant Support: Th s work was supported, n part, by grant UL-1-RR-25711 from the National Institutes of Health and by the Mushroom Council.
Potential Competing Interests: Dr Holick is a consultant for Quest Diagnostics, Ontometrics, Vital Choice, Merck, and Bioceuticals.
Correspondence: Address to Michael F. Holick, PhD, MD, Boston University School of Medicine, 85 E Newton St, M-1013, Boston, MA 02118 ([email protected]).
REFERENCES in PDF
Main points of the study from: Integrated Health Blog
Vitamin D deficiency is common and underdiagnosed.
An effective strategy to prevent Vitamin D deficiency and insufficiency is to obtain some sensible sun exposure, ingest foods that contain Vitamin D, and take a Vitamin D supplement.
Evidence from hundreds of recent studies suggests that Vitamin D is important for reducing the risk of type 1 diabetes mellitus, cardivascular disease, certain cancers, cognitive decline, depression, pregnancy complications, autoimmunity, allergy, and frailty.
Vitamin D deficiency during pregnancy may influence fetal “imprinting” that may affect chronic disease susceptibility shortly after birth, as well as later in life.
The blood level of 25(OH)D is the best method to determine Vitamin D status.
Note: lots more on the study and on vitamin D at Integrated Health Blog
Short url =http://is.gd/Holick613