Vitamin D Is Not as Toxic as Was Once Thought – Holick
Vitamin D Is Not as Toxic as Was Once Thought: A Historical and an Up-to-Date Perspective
MAYO CLINIC PROCEEDINGS May 2015 Volume 90 Number 5
Michael F. Holick, PhD, MD [email protected]
Section of Endocrinolog/, Diabetes and Nutrition Department of Medicine Boston University Medical Center Boston, MA
📄 Download the PDF from Vitamin D Life
In the current issue of Mayo Clinic Proceedings, Dudenkov et al1 report on a retrospective study of serum 25-hydroxyvitamin D (25(OH)D) values in patients registered in the Rochester Epidemiology Project. The article reported that although serum 25(OH)D values of more than 50 ng/mL increased over the 10-year study period, vitamin D toxicity and hypercalcemia were exceedingly rare. To understand the importance of this finding as it relates to clinical care, it is useful to begin with a review of the history of hypovitaminosis D diagnosis and vitamin D replacement, followed by new insights into vitamin D offered in the recent literature.
In the late 19th and early 20th centuries, there was evidence of the growth retardation and bony deformities associated with rickets in more than 80% of the children living in cities on the East Coast of the United States and in cities throughout Europe.2 In 1921, Hess and Unger reported that exposing children to sunlight was an effective treatment for rickets. This was quickly followed by the observation that exposure of various foods to ultraviolet radiation imparted antirachitic activity. This led to the addition of ergosterol to milk that was then exposed to ultraviolet B radiation, which resulted in the production of vitamin D2. With the discoveries of vitamin D2 and vitamin D3 and the development of methods to cheaply produce these vitamins, they were used to directly fortify milk with vitamin D.2 Children who drank vitamin D—fortified milk no longer developed rickets. As a result of this success, vitamin D fortification became widespread throughout the United States and Europe.2,3 Not only milk but a wide variety of foods and beverages were fortified with vitamin D, including bread, soda pop, beer, custard, and even hot dogs.2 In the 1940s, vitamin D was thought to be effective for treating rheumatoid arthritis and massive doses of 200,⑻0 to 300,⑻0 IU/d were given. It was soon realized that these massive doses resulted in vitamin D intoxication, including hypercalcemia, hyperphosphatemia, nephrocalcinosis, kidney stones, and soft tissue calcifications. When the vitamin D treatment was stopped, it took months to years for the manifestation of vitamin D intoxication to resolve because this fat-soluble vitamin (stored in body fat) continued to be released back into the circulation. Thus, physicians were alerted to the potential of vitamin D being toxic. However, these experiences did not influence the fortification of foods and other products with vitamin D, which persisted until the 1950s.
In Great Britain in the early 1950s, several cases of infants with facial abnormalities, supravalvular aortic stenosis, mental retardation, and hypercalcemia were reported.4 This was followed by reports of hypercalcemia as high as 19 mg/dL in some infants.3 The Royal College of Physicians and the British Pediatric Association were charged with finding the cause for these unusual occurrences. After careful scrutiny of the literature and surveys of dietary intake, they concluded that the most likely causes were the unregulated overfortification of milk with vitamin D and/or excessive intakes of vitamin D from various foods fortified with vitamin D and natural foods containing vitamin D, including dried milk and cod liver oil.3,5 Although the Royal Academy of Physicians admitted that it did not have any direct evidence for this conclusion, it based its conclusion on the literature that reported that pregnant rodents receiving intoxicating doses of vitamin D delivered pups with altered facial features, supravalvular aortic stenosis, and hypercalcemia.6 The British Pediatric Association documented hypercalcemia but only in a relatively few infants who had approximate intakes of 1500 to 1725 IU/d of vitamin D. As a result, legislation was instituted in Great Britain forbidding the fortification of any food or any product with vitamin D . This concern for vitamin D toxicity in children led to most of the world (including countries in Europe, the Middle East, Asia, Africa, and South America) banning vitamin D fortification of milk. Only the United States, Canada, and a few European countries continued to permit milk to be fortified with vitamin D. However, in retrospect, it is likely that these infants were suffering either from
the rare genetic disorder William syndrome , which is associated with elfin facies,
supravalvular aortic stenosis,
mental retardation, and
hypercalcemia due to a hypersensitivity to vitamin D,
or from other vitamin D hypersensitivity disorders
- including sarcoidosis and 24-hydroxylase deficiency.7-9
The historical underpinnings of contemporary perspectives on vitamin D toxicity are rarely appreciated, but the concept that vitamin D is one of the most toxic fat-soluble vitamins has been instilled in the psyche of health regulators and the medical community. Currently, there is great concern about the potential for the widespread increased use of vitamin D increasing the risk for kidney stones, cardiovascular calcifications, and even death.10,11
Vitamin D deficiency (25(OH)D level <20 ng/mL) and insufficiency (25(OH)D level 21-29 ng/mL) is a worldwide problem.12 The US Centers for Disease Control and Prevention reported that 33% of children and adults are at risk for vitamin D deficiency.13 Vitamin D is not only important for maximizing bone health but also has been implicated in reducing the risk for many chronic and acute diseases.2, With all the publicity surrounding the health benefits of vitamin D, health care professionals have begun to routinely measure serum 25(OH)D levels and treat their patients with vitamin D. However, the Institute of Medicine11 raised concerns about widespread vitamin D supplementation potentially causing harm. Of note, it found that vitamin D deficiency was associated with increased risk for mortality. However, it cautioned that when blood levels of 25(OH)D were more than 30 ng/mL, there was the potential for increased risk for mortality, and it cautioned that blood levels of 25(OH)D should not be more than 50 ng/mL.11
The current report of Dudenkov et al1 sheds light on the appropriateness of the Institute of Medicine recommendation. Dudenkov et al1 evaluated more than 20,000 25(OH)D measurements performed at Mayo Clinic from 2002 to 2011 and related blood levels of 25(OH)D of more than 50 ng/mL with potential vitamin D toxicity (as determined by the presence of hypercalcemia). They observed that from 2002 to 2011, there was a more than 20-fold increase in the number of individuals with serum 25(OH)D levels of more than 50 ng/mL; however, elevated serum 25(OH)D levels were not statistically significantly related to serum calcium values.
This discovery of Dudenkov et al1 is logical because the body tightly controls the conversion of 25(OH)D to 1,25-dihydroxyvitamin D, which is responsible for regulating calcium metabolism by enhancing intestinal calcium absorption and mobilizing calcium from the skeleton. A study of healthy adults who received 1000 IU of vitamin D3 daily for 11 weeks and who raised their blood levels of 25(OH)D from 22.2 土 13 to 33.6 土 7.5 ng/mL reported that blood levels of 1,25- dihydroxyvitamin D did not change: baseline, 35.4 土 13.0 pg/mL; 11 weeks later, 34.3 土 13.8 pg/mL.14 Dudenkov et al also found that only 1 person with a serum 25(OH)D level of 364 ng/ mL had evidence of clinical toxicity, that is, hypercalcemia. For comparison, the Endocrine Society’s practice guidelines on vitamin D state that vitamin D intoxication is usually not observed until serum 25(OH)D levels are more than 150 ng/mL.15
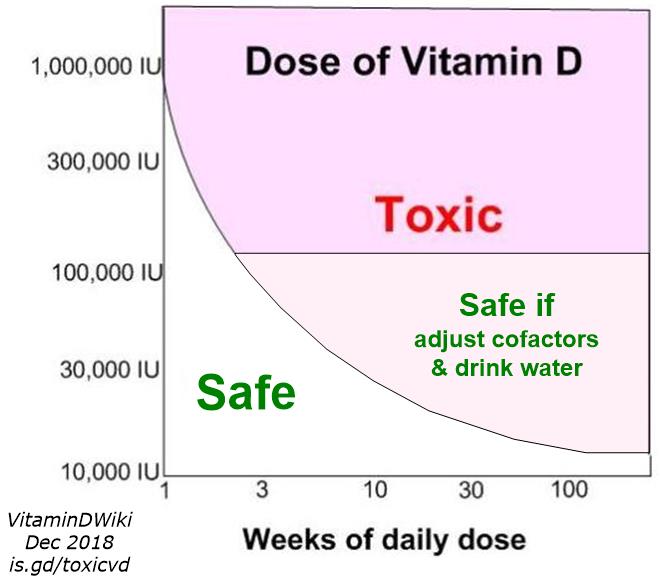
Vitamin D intoxication associated with hypercalcemia, hyperphosphatemia, and suppressed parathyroid hormone level is typically seen in patients who are receiving massive doses of vitamin D in the range of 50,000 to 1 million IU/d for several months to years. Ekwaru et al16 recently reported on more than 17,000 healthy adult volunteers participating in a preventative health program and taking varying doses of vitamin D up to 20,000 IU/d. These patients did not demonstrate any toxicity, and the blood level of 25(OH)D in those taking even 20,000 IU/d was less than 100 ng/mL. For point of reference, a 25(OH)D level of 100 ng/mL is considered by the Institute of Medicine, the Endocrine Society, and many reference laboratories to be the upper limit of normal.11,12,15
There remains concern, however, that increasing vitamin D intake even by 400 IU/d increases the risk for kidney stones, especially in patients with a history of kidney stones.10 Despite this concern, there is no credible scientific literature suggesting that such vitamin D intake increases the risk for kidney stones.12,15 Similarly, data are weak regarding the association between vitamin D intake and cardiovascular calcifications.12 To the contrary, current evidence suggests that improvement in vitamin D status reduces the risk for hypertension, stroke, and myocardial infarction.12
There also remains concern that increasing vitamin D intake and raising blood levels of 25(OH)D result in a U curve for mortality risk; that is, when blood levels of 25(OH)D are more than 30 ng/mL, there is a slight increase in mortality.11 Is it possible that those with blood levels of 25(OH)D of more than 50 ng/mL were being treated for vitamin D deficiency and therefore retained their increased risk for mortality because of their chronic vitamin D deficiency rather than because their blood level of 25(OH)D was more than 50 ng/mL? The observation by Dudenkov et al1 clearly demonstrated that likely because of an increase in the treatment of vitamin D deficiency, there was, over a 10-year period, a more than 20-fold increase in the number of patients with a blood level of 25(OH)D of more than 50 ng/mL.
On the basis of the Dudenkov et al report, we cannot be sure whether it is vitamin D prescription by physicians or patients’ self administration of large doses of vitamin D that resulted in serum 25(OH)D levels of more than 50 ng/mL. The research of Kroll et al17 may provide some insights. They evaluated 3.8 million 25(OH)D laboratory results of adults. They not only reported that 33% and 60% of the samples were less than 20 and less than 30 ng/mL, respectively, but also that a significant number of samples were more than 50 ng/mL. They used a liquid chromatography tandem mass spectroscopy assay and were able to independently measure levels of 25(OH)D2 and 25(OH)D3. Because most vitamin D supplements and calcium supplements containing vitamin D contain vitamin D3, and there is essentially no vitamin D2 in the diet unless sun-exposed or ultraviolet-exposed mushrooms are ingested, the presence of 25(OH)D2 in the sample is suggestive of the patient being treated for vitamin D deficiency. The reason is that the only Food and Drug Administration—approved pharmaceutical form of vitamin D available in the United States is vitamin D2. Physicians are now routinely treating patients with 50,000 IU of vitamin D2 as recommended by the Endocrine Society’s practice guidelines.15 In the research of Kroll et al,17 evaluation of all the samples that had blood levels of 25(OH)D of more than 50 ng/mL revealed that 57% had detectable levels of 25(OH)D2. This suggests that most of the individuals who had 25(OH)D levels of more than 50 ng/mL had such levels because they were being treated by a physician for vitamin D deficiency.
The Endocrine Society’s practice guidelines suggest daily vitamin D supplementation of 400 to 1000, 600 to 1000, and 1500 to 2000 for ages 0 to 1 year, 1 to 18 years, and all adults, respectively.15 (Obese adults require doses 2-3 times higher.) However, there are clinical circumstances that can cause hypercalcemia when giving patients these recommended doses of vitamin D. These conditions include patients with granulomatous disorders including sarcoidosis, William syndrome, some lymphomas, and the rare genetic disorder of the absence of the 25-hydroxyvitamin D-24- hydroxylase.2,6,9,12,15
The evidence is clear that vitamin D toxicity is one of the rarest medical conditions and is typically due to intentional or inadvertent intake of extremely high doses of vitamin D (usually in the range of >50,000-100,000 IU/d for months to years).12 Glucocorticoids have been routinely used to treat patients with vitamin D intoxication. However, the adverse effects of treatment can be considerable, including the increased risk for gastrointestinal bleeding, aseptic necrosis of the hip, and infectious diseases. Simply reducing the calcium intake, wearing sun protection to prevent vitamin D production, and eliminating all vitamin D from dietary sources will result in a gradual decrease in serum 25(OH)D levels, with no significant sequelae from the toxicity.2,12
REFERENCES
DudenkovDV,YawnBP,〇be「helmanSS,etal.Changinginci- dence ofse「um25-hyd「oxyvitamin Dvaluesabove50 ng/mL: a 10 year population-based study. Mayo GinProc.20l5;90(5): 577-586.
Wacker M, Holick MF. Sunlight and vitamin D: a global perspective fo「 health. Dermatoendoo7.no/. 20l3;5(l):5l-l08.
Stapleton T, MacDonald WB, Lightwood R. The pathogenesis of idiopathic hypercalcemia in infancy. Am J C/in Nutr. l957; 5(5):533-542.
Palermo NE, Holick MF. Vitamin D, bone health, and other health benefits in pediatric patients. J Pediatr Rehab./ Med. 20l4;7(2):l79-l92.
Samuel HS. Infantile hypercalcaemia, nutritional rickets, and infantile scurvy in Great Britain: a British Paediatric Association ^port. Br Med J. l964;l(5399):l659-l66l.
Friedman WF, Roberts WC. Vitamin D and the supravalvular aortic stenosis syndrome: the transplacental effects of vitamin D on the aorta of the rabbit. Grcu/at/on. l966;34:77-86.
Pober BR. Williams-Beuren syndrome. N Eng/ J Med. 20l0; 362(3):239-252.
Taylor AB, Stern PH, Bell NH. Abnormal regulation of circulating 25-hydroxyvitamin D in the Williams syndrome. N Eng/ JMed. l982;306(l6):972-975.
Schlingmann KP, Kaufman M, Weber S, et al. Mutations in CYP24 Al and idiopathic infantile hypercalcemia. N Eng/ J Med. 20ll;365(5):4l0-42l.
Jackson RD, LaCroix AZ, Gass M, et al. Calcium plus vitamin D supplementation and the risk of fractures. N Eng/ J Med. 2006; 354(7):669-683.
Ross AC, Manson JE, Abrams SA, et al. The 20ll report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J C/in Endo- cr.no/ Metab. 20ll;96(l):53-58.
Hossein-nezhad A, Holick MF. Vitamin D for health: a global perspective. Mayo C/in Proc. 20l3;88(7):720-755.
Looker AC, Johnson CL, Lachner DA, Pfeiffer CM, Schleicher RL, Sempos CT. Vitamin D Status: United States, 200l-2006. NCHS Data Br/e/: 20ll;(59):l-8.
Biancuzzo RM, Clarke N, Reitz RE, Travison TG, Holick MF. Serum concentrations of l,25-dihydroxyvitamin D2 and l,25- dihydroxyvitamin D3 in response to vitamin D2 and vitamin D3 supplementation. J C//n Endocr/no/ Metab. 20l3;98(3):973-979.
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J C/in Endocrino/ Metab. 20ll;96(7):l9ll-l930.
Ekwaru JP, ZwickerJD, Holick MF, Giovannucci E, Veugelers PJ. The importance of body weight for the dose response relationship of oral vitamin D supplementation and serum 25-hydroxy- vitamin D in healthy volunteers. PLoS One. 20l4;9(ll):elll265.
Kroll MH, Bi C, Garber CC, et al. Temporal relationship between vitamin D status and parathyroid hormone in the United States. PLoS One. 20l5;l0(3):e0ll8l08.
Vitamin D Life pages with HOLICK in title (47 as of April 2022)
This list is automatically updated
{LIST()}