Vitamin D papers from European Vitamin D Association Conference
Most of the ENGLISH presentations of the conference follow
Polish Presentations and Polish abstracts are in the [dl3144]
Graphics and table are generally in the [dl3144]
References are generally in the [dl3144] as well
Vitamin D Update 2015: What We Need to Know about Its Health Benefits and Potential for Toxicity?
Michael F. Holick
Boston University Medical Center, Boston
For more than 40 years the sun has been reviled for its cancer promoting properties and thus avoidance of any direct sun exposure has been widely promoted by many healthcare organizations and government agencies. The lack of appreciation that sun exposure had been the major source of vitamin D for children and adults worldwide has led to a vitamin D deficiency pandemic. This pandemic has been associated with a wide variety of chronic diseases as well as increased risk for mortality. There continues to be paranoia about the potential for vitamin D toxicity which has resulted in the banning of vitamin D fortification and tight government regulations on vitamin D supplementation in most countries in the world. To conquer this world wide health issue there needs to be:
A recognition that sensible sun exposure can provide children and adults with the sunshine vitamin D;
Vitamin D is not toxic in amounts that could be used in food fortification;
Until the first two recommendations are instituted there is a need to recognize that most children and adults need to receive adequate vitamin D supplementation throughout the year.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 112-116
Introduction
Vitamin D is now the most talked about nutrient by both healthcare professionals and the lay press. Although many naysayers have suggested that the hype surrounding vitamin D would eventually fade and go the way of the vitamin E and vitamin A craze vitamin D has sustained its visibility as being one of the most important nutrients for overall health and well-being for more than a decade. More than 30,000 publications having been published many associated with a variety of health benefits in the past 10 years. Vitamin D is one of the oldest hormones on this earth with it being documented to have been produced more than 500 million years ago in some of the earliest phytoplankton life forms1'2. Vitamin D established itself as being critically important for the evolution of vertebrates since it was responsible for enhancing the efficiency of dietary calcium thereby maintaining circulating calcium concentrations within a physiologically acceptable range. Calcium combining with phosphate also provided the major component of the skeleton that provided strength to the bones to sustain its structural integrity permitting them to ambulate in their 1 G environment. Remarkably this vital nutrient is naturally provided to vertebrates including humans during sun exposure. Once formed in the skin vitamin D begins its journey into the bloodstream entering the liver to undergo its first obligate hydroxylation on carbon 25 to generate the major circulating form 25-hydroxyvita- min D [25(OH)D]. This metabolite is bound to the vitamin D binding protein (DBP) and is transported to the kidneys where through a megalin facilitated transport both the binding protein and 25-hydroxyvitamin D enter into the renal tubule where it undergoes its final activation step and converted to 1'25-dihydroxyvitamin D3 [1'25(OH)2D3]2. Once formed it enters the circulation and travels to the small intestine where it interacts with its nuclear vitamin D receptor (VDR) to influence a variety of genes that results in an increase in intestinal calcium absorption. 1'25(OH)2D3 also travels to the skeleton where it interacts with the VDR in osteoblasts increasing the genomic expression of RANKL. This ligand interacts with its receptor RANK on monocytes inducing them to aggregate together forming a multi nucleated osteoclast which in turn mobilizes calcium from the skeleton1'2.
It is now recognized that most tissues and cells in the body have a VDR and that many cells and tissues also expressed the 25-hydroxyvitamin D-1 alpha-hydroxylase thus providing them with the enzymatic machinery to locally produce 1,25(OH)2D. It has been hypothesized that it is the local production of 1,25(OH)2D which is thought to regulate upwards of 2000 genes is responsible for many of the noncalcemic health benefits ascribed to improvement in vitamin D status3. It is been reported that 1,25(OH)2D modulates cellular growth and differentiation, enhances the production of cathelicidin, modulates both T and the lymphocyte activity, stimulates insulin production among other biologic activities. These observations help explain the association with improvement in vitamin D status with reduced risk for many deadly cancers, autoimmune diseases including multiple sclerosis and type 1 diabetes, cardiovascular disease and stroke, neurocognitive dysfunction including Alzheimer’s disease, infectious diseases including influenza and tuberculosis and type 2 diabetes2. Because 1,25(OH)2D is such a potent hormone in regulating calcium metabolism, to prevent the escape of 1,25(OH)2D from these extra renal cells into the circulation which could potentially cause hypercalcemia and serious health consequences, as 1,25(OH)2D is regulating gene activity for a variety of biologic functions it also at the same time induces the 25-hydroxyvitamin D-24-hydroxylase. This multi-functional enzyme2,4 is responsible for hydroxylating and oxidizing the side arm of 1,25(OH)2D to produce a biologically inactive water soluble calcitroic acid.
There has been a lot of discussion about what defines vitamin D deficiency and insufficiency. There is concern about health cost associated with measuring blood levels of 25(OH)D. Neither the Institute of Medicine nor the Endocrine Society as well as many medical societies recommend the broad screening for vitamin D status in otherwise healthy children and adults5,6. With all the hype about the health benefits of vitamin D the use of vitamin D supplements by children and adults worldwide has markedly increased. This has raised concerns about the potential for increased risk for kidney stones and vitamin D toxicity. The goal of this review will be to put these issues into perspective.
How Much Vitamin D to Children and Adults Require for Health
Before 2010 it was generally accepted that the RDA for vitamin D for all children and adults up to the age of 50 was 200 IUs daily5-7. This was based on the fact that it was thought that vitamin D deficiency was not a health issue and was based on the work of Jeans in the 1940s who demonstrated that 100 IUs of vitamin D was sufficient to prevent overt skeletal consequences of rickets6. The Institute of Medicine recognized that this was inadequate based on more current literature and recommended that to maintain a blood level of 25(OH)D of at least 20 ng/mL that infants required 400 IUs daily, children 1 year and older and adults 600 IUs daily and adults over the age of 70 800 IUs daily5. The Endocrine Society whose goal was to make recommendations to treat and prevent vitamin D deficiency and to achieve a blood level of 25(OH)D>30 ng/mL the preferred range of 40-60 ng/mL recommended that infants up to 1 year needed 400-1000 IUs daily, children over 1 year 600-1000 IUs daily and all adults 1500-2000 IUs daily. For those with a BMI >30 day required to-3 times more to satisfy that requirement8.
How Much Vitamin D Causes Toxicity and What Are the Consequences?
It is generally accepted that a blood level of 25(OH)D of up to 100 ng/mL is perfectly safe for most children and adults with the exception of those who have a hypersensitivity to vitamin D including children and adults with William’s syndrome, granulomatous disorders and some lymphomas8. The Endocrine Society concluded that vitamin D toxicity is not only extremely rare but that a blood level of at least 150 ng/mL would be required before there would be any evidence of vitamin D toxicity. The first manifestation of excess vitamin D activity is increased excretion of urinary calcium due to a decrease in the parathyroid hormone (PTH) production. When the kidneys can no longer keep up with the amount of calcium entering into the circulation from dietary calcium and bone calcium mobilization the serum calcium begins to rise. The decrease in PTH also causes a decrease in phosphate excretion by the kidneys. The elevated levels of 25(OH)D directly interacts with the VDR in the intestine increasing intestinal calcium and phosphate absorption. This results in an increase in both serum calcium and serum phosphate resulting in a supra saturating calcium phosphate product which is deposited in the kidneys resulting in nephrocalcinosis and in atherosclerotic plaques in blood vessels leading to vascular calcification. The hypercalcemia also results in vasoconstriction that can cause hypertension. The hypercalcemia causes a variety of nonspecific symptoms including constipation, confusion, polyuria and polydipsia as well as cardiac arrhythmias1'5.
Vitamin D toxicity remains as a major concern for obstetricians, neonatologist, pediatricians, internist as well as public health government agencies. This is the major reason why most countries in the world do not permit fortification of foods such as milk with vitamin D. Before the 1950s there was widespread fortification of vitamin D since it was considered to be one of the miracle nutrients that was useful for treating many chronic illnesses from tuberculosis to rheumatoid arthritis. Indeed besides milk being fortified with vitamin D so too was custard in England, beer in the United States, shaving cream and soap in Germany fortified with this fat-soluble vitamin. However in the early 1950s several cases of infants with facial abnormalities, supravalvular aortic stenosis, mental retardation and hypercalcemia were reported in Great Britain. This was followed by additional reports of hypercalcemia as high as 19 mg/dL in some infants also in Great Britain9. The Royal College of Physicians and the British Pediatric Association were charged with finding the cause for these horrific events. After careful scrutiny of the literature and surveys of dietary intake they concluded that the likely causes were due to the unregulated over fortification of milk with vitamin D as well as excessive intakes of vitamin D from various foods fortified with vitamin D and natural foods containing vitamin D. Although the Royal College of Physicians admitted that it did not have any strong evidence for this conclusion they based their conclusion on literature reporting that pregnant rodents that received high doses of vitamin D delivered pups with altered facial features, supravalvular aortic stenosis and hypercalcemia. The British Pediatric Association documented hypercalcemia but only in a relatively few infants who had approximate intakes of 15001725 IUs daily. At this time there was no reliable assay for vitamin D so these intakes were at best guesstimates. It is likely that some of these infants had a William’s syndrome which is associated with elfin facies, aortic stenosis, mental retardation and hypercalcemia due to a hypersensitivity to vitamin D10,11. Since these infants had evidence for mental retardation this cause great consternation for both parents and politicians and without further consideration passed laws forbidding not only the fortification of milk and other foods with vitamin D but any and every product potentially used by a child or adult including skin creams. This hysteria spread throughout Europe and ultimately around the Globe and most government agencies also put in place laws forbidding the fortification of foods with vitamin D. They also instituted policies to strictly regulate vitamin D supplements available to the general public. Many countries in Europe, Asia and South America forbid the availability of vitamin D supplements to the general population. The only way that children and adults in some countries are able to receive any supplemental vitamin D is through their doctor10.
There are numerous studies demonstrating that vitamin D is probably one of the least toxic fat-soluble vitamins certainly much less toxic and vitamin A. Dudenkov et al12. evaluated more than 20,000 25(OH)D measurements performed at Mayo Clinic from 2002 to 2011 and related blood levels of 25(OH)D with potential vitamin D toxicity (determined by presence of hypercalcemia). Whereas they observed a 20-fold increase in the number of individuals with a serum 25(OH)D>50 ng/mL these levels were associated with a normal serum calcium. They found only one person having hypercalcemia and the blood level was 364 ng/ML. Pietras et al13. reported that healthy adults in a clinic setting receiving 50,000 IUs of vitamin D2 once every 2 weeks (equivalent to approximately 3300 IUs daily) for up to 6 years maintaining blood levels of 25(OH)D in the desired range of 40-60 ng/mL without any evidence of toxicity. This was also consistent with the observation by Ekwaru et al14. who reported in some Canadian adults who ingested up to 20,000 IUs of vitamin D3 daily raise their blood levels of 25(OH)D into the 60 ng/mL range without any toxicity. They also confirmed what was recommended by the Endocrine Practice Guidelines that obese adults require 2.5 times as much vitamin D supplementation to maintain the blood level of 25(OH)D in the same range as a normal weight person7.
The Ominous J-U Curve for Mortality
There have been a multitude of studies evaluating serum 25(OH)D with risk of chronic illnesses as well as mortality. Several of the studies that have plotted serum 25(OH)D versus a chronic illness for mortality observed that vitamin D deficiency was associated with an increased risk and that this risk gradually decreased with increasing levels of 25(OH)D that reached a nadir plateau that was usually between 30-40 ng/mL. However there appeared to be a slight increase in risk for the chronic illness or mortality when blood levels were approaching 50 ng/mL raising concerns that there was the potential for negatively impacting health if these levels were attained with vitamin D supplementation. The Institute of Medicine suggested that there could be an increase in risk for mortality when blood levels of 25(OH)D began to increase above 30 ng/mL6. What is remarkable is that the conclusions were made based on essentially no information for those who had circulating blood levels of 25(OH)D above 50 ng/mL. It has been documented that Ma- asai Warriors outside every day reach blood levels of approximately 50 ng/mL15. Diet is incapable of providing an adequate amount of vitamin D3 on a daily basis. Thus without being exposed to sunlight essentially every day it’s not possible to achieve a blood level of 25(OH)D of 50 ng/mL unless the person has a 24-hydroxylase deficiency4,16. Thus it’s more likely that subjects in studies relating serum 25(OH)D levels with mortality or chronic disease who have blood levels above 50 ng/mL are being treated with vitamin D for their vitamin D deficiency. Without any knowledge of the vitamin D intake of subjects for most of the studies it was next to impossible to determine this as a potential explanation. However Kroll et al17. mined the database at Quest Diagnostics and retrospectively determined population weekly-mean concentrations of 25(OH)D2 and 25(OH)D3 and PTH in 3.8 million laboratory results of adults. They observed for all genders and latitudes 25(OH)D3 peaks occurred in September and troughs in March. The PTH levels showed an inverse pattern of peaks and troughs relative to 25(OH)D3 with a delay of 4 weeks. In the United States only vitamin D2 is available as a pharmaceutical to treat and prevent vitamin D deficiency. There is essentially no vitamin D2 from dietary sources; the major source being sun-dried mushrooms. Indeed 69.4% of the samples had no detectable 25(OH)D2. This is consistent with a multitude of studies published throughout the world using the Gold standard LC MS MS 25(OH)D assay which reports that essentially none of the samples contained detectable 25(OH)D2. It was surmised that those adults in the United States with detectable 25(OH)D2 were being treated for vitamin D deficiency. In fact of patients with a total 25(OH)D > 50 ng/mL 57% had detectable 25(OH)D2.
This suggested that they were being treated for vitamin D deficiency. Thus it would not be at all unexpected that they would still retain their higher risk for chronic illness and mortality due to their vitamin D deficiency. Recently Garlandet. al18. conducted a meta-analysis and found like other studies that vitamin D deficiency was associated with a higher risk for mortality and that this mortality gradually declined to a nadir plateau at around 40 ng/mL that was sustained up to at least 70 ng/mL with no evidence of a U or J-shaped curve.
Conclusion
It is now recognized that vitamin D deficiency and insufficiency is a Global health problem. On average 40% of children and adults have blood levels of 25(OH)D<20 ng/mL and 60%<30 ng/mL1'19. The consequences of this Global vitamin D deficiency pandemic is having catastrophic consequences on the health and welfare of children and adults. It has been estimated that there could be a 25% reduction in most healthcare costs that it been related with diseases that have been associated with vitamin D deficiency and insufficiency. The major causes are
Lack of appreciation that sensible sun exposure is a safe and inexpensive way of obtaining vitamin D naturally;
Contrary to popular belief very few foods naturally contain vitamin D and therefore a healthy diet will not provide an adequate amount to satisfy the body’s requirement and
The concern by health authorities and healthcare professionals that vitamin D is an extremely toxic fat-soluble vitamin and therefore needs to be highly regulated.
The solution to conquer this health crisis is for the health authorities and legislative bodies implement supplementation of foods such as milk, bread and pasta with vitamin D. Instead of demonizing the sun which has occurred for the past 40 years there needs to be recognition that sensible sun exposure can be a major safe source of vitamin D for most children and adults20. The use of the free app dminder.info, that I helped develop, provides information as to when and where vitamin D production will result from exposure to sunlight and warns the user after sensible sun exposure to seek sun protection to prevent sun burning. Finally to guarantee vitamin D sufficiency I recommend to all of my friends, family and patients that children should take 1000 IUs vitamin D daily, teenagers and adults 2000 IUs daily and for those who are obese with a BMI >30 4000-5000 IUs daily. ■
[Skin synthesis of vitamin D - pros and cons] English Abstract
Nearly all cells and organs of human body are adapted to using the active form of vitamin D as a co-regulator of many important physiological pathways and as an enhancer of their normal actions. Insufficient vitamin D status has been proven to be a source of perturbances in mineral metabolism resulting in rickets and osteomalatia. There are also reasons to believe that vitamin D insufficiency and deficit, underlies such problems as certain kinds of cancer, kidney and heart diseases, diabetes, high blood pressure, obesity, fractures, osteoporosis, dental problems, respiratory tract infections, and central nervous system malfunctions.
Human body has been adopted during the evolution to use skin synthesis as the main source of vitamin D. As a result, this process has become a difficult to replace component of the vitamin D supplementation system for the contemporary human body especially in societies living far from the equator. There are well founded stipulations for using the solar ultraviolet rays as a stimulant of vitamin D synthesis as it is known that this can promote dangerous skin cancers. It is also known that this can be avoided by applying „reasonable" rudiments and avoiding the excessive exposition to sun rays.
Nutritional Rickets - global guidelines for prevention and treatment
Tom D. Thacher1, Paweł Płudowski2, Mairead Kiely34
Mayo Clinic, Rochester, Minnesota, USA
Department of Biochemistry, Radioimmunology and Experimental Medicine, The Children's Memorial Health Institute, Warsaw, Poland
Vitamin D Research Group, School of Food and Nutritional Sciences, University College Cork, Ireland
Irish Centre for Fetal and Neonatal Translational Research (INFANT), University College Cork, Ireland
Nutritional rickets has reemerged as an important childhood public health problem with potentially life-threatening consequences and disability. The increasing burden of disease is disproportionately borne by immigrant populations, ethnic minorities, and by those in low income countries. This situation is completely preventable with adequate vitamin D and calcium intakes. Global consensus guidelines for the treatment and prevention of nutritional rickets have been recently published. Nutritional rickets is indicative of widespread vitamin D and calcium deficiencies. The two most effective interventions for prevention of nutritional rickets are infant vitamin D supplementation and food fortification.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592
KEY WORDS: ■ NUTRITIONAL RICKETS ■ GLOBAL GUIDELINES ■ VITAMIN D ■ CALCIUM ■ PREVENTION AND TREATMENT
Despite being nearly eradicated during the 20th century, nutritional rickets has been reemerging as a disease affecting child health in both high and low income countries. Presented here is a summary of recent guidelines that were developed by 33 experts at the Global Consensus Conference on the Treatment and Prevention of Nutritional Rickets, Birmingham, UK, May 2014 [ref ePub]. This group conducted a systematic review of the literature and graded the quality of evidence for each guideline recommendation1. The guidelines were targeted to clinicians caring for children at risk of nutritional rickets and to health policy makers who can implement the public health recommendations.
THESES
Nutritional rickets has reemerged as an important public health problem worldwide.
Treatment and prevention of nutritional rickets requires adequate intakes of both vitamin D and calcium.
The most effective public health interventions for prevention of nutritional rickets are infant vitamin D supplementation and food fortification.
Nutritional rickets can result in the deformity of growing bones, bone pain, impaired growth, developmental delay, chest wall deformity, hypocalcemic seizures, and potentially fatal cardiomyopathy2-4. Although children with rickets have an increased risk of fracture5'6, children with vitamin D deficiency in the absence of rickets have no evidence of an increased fracture risk7. The diagnosis of rickets is based upon recognition of the clinical presentation. Biochemical features associated with nutritional rickets include an elevated alkaline phosphatase, low serum phosphorus and calcium, and elevated PTH. Serum vitamin D levels are variable, depending on the cause. Radiographs, typically of the wrists and knees, are needed to confirm the diagnosis of active rickets8.
Adequate bone mineralization depends upon both sufficient vitamin D and calcium. Nutritional rickets can result from inadequate vitamin D status, as reflected by low serum 25(OH)D concentration, or inadequate dietary calcium intake. The interaction of vitamin D and calcium to maintain bone mineralization is such that an adequate intake of either one will generally compensate for suboptimal intake of the other. However, when both calcium intake and vitamin D status are low, rickets can develop9. Rickets resulting from vitamin D deficiency is generally associated with serum 25(OH)D values < 30 nmol/L, and serum 25(OH)D > 50 nmol/L is targeted as sufficient for the purpose of preventing nutritional rickets.
Ultraviolet B (UVB) radiation from sunlight leads to the epidermal synthesis of vitamin D. Although restricted sun exposure is a risk factor for vitamin D deficiency and nutritional rickets, no safe threshold of ultraviolet light exposure that will maintain adequate 25(OH)D levels across the population can be recommended without increasing skin cancer risk. Several risk factors are associated with vitamin D deficiency and nutritional rickets. A latitude > 35°, which includes most of Europe and North America, results in virtually no UVB radiation exposure during winter months. People with dark skin pigmentation require longer UVB exposure to produce the same amount of vitamin D than those with white skin, and the vast majority of cases of rickets occur in children with dark skin10,11. Limited UVB exposure results from children kept indoors, covering by clothing,12 cloud cover, air pollution,13 or sunscreen use. Maternal vitamin D deficiency results in neonates beginning life vitamin D deficient. Because breast milk has very limited concentrations of vitamin D, prolonged breast feeding can lead to rickets, unless the infant has adequate supplementation or complementary foods with vitamin D and calcium10,14.
Nutritional rickets is common in tropical countries of Africa and the Indian subcontinent, where sunlight is abundant, but calcium intakes are low15-17. Dietary calcium intakes < 300 mg/d increase the risk of rickets, independent of vitamin D status. In contrast to vitamin D-deficiency rickets, which most commonly presents in the first year of life, calcium-deficiency rickets presents after the first year in settings where dairy product intake is limited. The dietary calcium intakes that are adequate to prevent nutritional rickets vary by age. During infancy, the infant’s calcium requirements can be met by exclusive breast feeding or formula, 200 mg/d and 260 mg/d of calcium, for infants ages 0-6 and 6-12 months, respectively18. Beyond age 12 months, a calcium intake of 500 mg/d throughout childhood is sufficient to prevent rickets19, and complementary foods rich in calcium should be introduced to meet this target.
Vitamin D 400 IU/d in infancy and childhood is sufficient to prevent nutritional rickets and vitamin D deficiency in otherwise healthy infants with an adequate calcium intake6,20,21. In the first year of life, all infants should receive supplementation. After 12 months of age, children should meet their requirement of 600 IU/d through diet and/or supplementation to prevent nutritional rickets. These intakes are sufficient to raise 25(OH)D concentrations above 50 nmol/L in healthy children, and routine screening of serum 25(OH)D is not recommended. Because few foods naturally contain vitamin D, vitamin D supplementation should be provided in the absence of food fortification, particularly to children and pregnant women at increased risk of vitamin D deficiency.
Vitamin D toxicity is defined as hypercalcemia with serum 25(OH)D > 250 nmol/L, associated with hy- percalciuria and low PTH levels. However, vitamin D toxicity rarely occurs unless 25(OH)D values are above 500 nmol/L22. Mutations of the CYP24A1 gene encoding the 24-hydroxylase enzyme, which degrades the active form of vitamin D, can result in infantile hypercalcemia with vitamin D supplementation23.
The minimum recommended doses of vitamin D and calcium given orally for treatment of nutritional rickets are vitamin D 2000 IU/d and elemental calcium 500 mg/d. With regard to vitamin D, daily doses of vitamin D2 or D3 are equally effective but vitamin D3 may be preferred for single large doses, because of its longer half-life24. Vitamin D should be given orally rather than by intramuscular injection25,26. Nutritional rickets should be treated for at least 12 weeks and healing confirmed radiographically27. Some children require a longer duration of treatment.
Neonatal cord blood 25(OH)D levels are directly related to but lower than maternal levels at birth28,29. Women of childbearing age should have a minimum vitamin D intake of 600 IU/d, including during pregnancy, in order to prevent congenital rickets and provide adequate vitamin D stores in the neonate. It is unclear if maternal supplementation with vitamin D has an effect on birth anthropometry, subsequent growth, or acquisition of bone mass29-31. Lactating women should maintain a vitamin D intake of 600 IU/d, but breast milk does not contain adequate vitamin D to meet the infant’s requirements, and infant supplementation is required. Although some studies indicate that breast milk can be enriched with high maternal doses of vitamin D, the safety of this approach has not yet been established32,33. Maternal calcium intake during pregnancy or lactation is not associated with breast milk calcium concentrations or neonatal bone mass. Consequently, calcium intakes in pregnant or lactating women do not need to exceed those recommend for non-pregnant women.
Public health strategies for prevention of nutritional rickets at a population level first require an assessment of the burden of disease and the magnitude of the problem. The burden of nutritional rickets can be measured by the severity of health consequences related to the disease and by its incidence and prevalence. Population-based samples can be used where the prevalence is expected to be high. Making rickets a mandatory reportable disease permits estimation of both prevalence and incidence in low prevalence regions. Case reports from designated sentinel centers can be used to estimate the incidence of new cases in a population.
A uniform case definition of nutritional rickets is needed for screening. Screening should be based on clinical features, followed by radiographic confirmation of suspected cases, because radiographs are the gold standard for diagnosis of active rickets. However, population screening with serum 25-hydroxyvitamin D, alkaline phosphatase, or radiographs is not indicated.
Public heath interventions should be tailored to regional prevalence and incidence. The prevalence of nutritional rickets is greatest in Asia, the Middle East and Africa, ranging from 1 to 24% of children34-37. Nutritional rickets has reemerged in high-income countries, with incidence figures ranging from 3 to 120 per 100,000 children6,10,38. In high-income countries, the incidence among Caucasian populations is stable or decreasing, and the overall increase in the incidence of rickets corresponds with an increase in ethnic minority, immigrant, and refugee populations. Little is known about the prevalence of the acutely life-threatening complications of nutritional rickets, like hypocalcemia and cardiomyopathy3. Nutritional rickets and its consequences need to be recognized as preventable global public health problems. Nutritional rickets can be considered the “the tip of the iceberg,” and its resurgence indicates widespread vitamin D or calcium deficiencies. The impact of nutritional rickets needs to be addressed as both a clinical and public health issue39. This requires educating clinicians, policy makers, and the public about the clinical presentation of rickets, its consequences, and the importance of adequate vitamin D and calcium intakes.
Rickets prevention programs will have the greatest impact in populations with a high prevalence of vitamin D deficiency, limited calcium intakes, or nutritional rickets. These programs can use a targeted approach to reach high risk groups of the population, or they can take a universal approach to cover all members of the population. A combination of the two approaches is most effective. Programs to universally supplement all infants with vitamin D 400 IU/d from birth to 12 months of age, independent of their mode of feeding, will prevent nutritional rickets. Beyond 12 months, groups at risk should continue vitamin D supplements. Vitamin D supplementation should be incorporated into existing childhood primary health care programs and antenatal care programs, which are already designed to provide recommended micronutrients and immunizations. Giving supplements is the fastest way to improve the micronutrient status of individuals or targeted populations40.
Daily oral vitamin D supplementation of infants and mothers effectively improves their vitamin D status41,42, but adherence is the primary obstacle with this approach. Vitamin D can be given in single large doses (for example, 50,000 IU every 2 months) as part of an immunization program43. This is similar to the use of high dose vitamin A supplementation in developing countries to prevent morbidity from measles. The effects of a single dose of vitamin D can last for 3 months or more, and this approach may be preferred when adherence is problematic.
A universal strategy that impacts all members of the population is food fortification with vitamin D. Vitamin D is found in a limited number of foods, and apart from fortified foods, dietary intakes have little impact on vitamin D status. Fortifying commonly consumed staple foods with vitamin D and calcium based on dietary patterns safely provides adequate intake to prevent deficiency at minimal cost. Food fortification can prevent rickets and improves the vitamin D status of children44,45. Following vitamin D fortification of milk in North America and of milk, margarine and cereals in the UK, the prevalence of rickets dramatically declined, so much so that it was considered almost eradicated46. Inadequate dietary calcium intake is a risk factor for nutritional rickets in children over the age of 12 months with low dairy product intake, a common situation in low income countries. In areas with inadequate calcium intakes, indigenous food sources of calcium or food fortification with calcium should be promoted or subsidized37'47. Calcium carbonate for food fortification is available at very low cost and can be used to fortify infant formulas, complementary and staple foods.
Successful food fortification requires that appropriate staple foods are selected, which will vary depending on socioeconomic, cultural and geographic factors48. Sufficient fortification needs to be provided to ensure that at-risk groups approach dietary recommendations49. Relevant legislation must support food fortification, and monitoring of the fortification process is required.
To determine the effectiveness of public health interventions, adherence to recommended vitamin D and calcium intakes needs to be monitored and surveillance for cases of nutritional rickets should be implemented. Successful vitamin D supplementation in Turkey resulted from training parents how to give vitamin D, explaining the benefits, and continuous monitoring and evaluation. As a result the prevalence of rickets declined from 6% to 0.1%, demonstrating the success of an infant vitamin D supplementation program. The cost-effectiveness of supplementation and food fortification programs needs further study in order to bolster the adoption of public health interventions.
TAKE HOME MESSAGES
Nutritional rickets has serious health consequences but is entirely preventable.
Public health strategies to ensure adequate vitamin D and calcium intakes are critical to eradicate the disease.
Targeting at-risk groups and case identification are essential to assess the population burden of the disease and monitor the effectiveness of rickets prevention efforts.
The role of vitamin D supplementation in treating health conditions and diseases common among those with intellectual and/or developmental disabilities
William B. Grant
Sunlight, Nutrition, and Health Research Center, San Francisco
People with intellectual and/or developmental disabilities often have low vitamin D concentrations from staying indoors. This situation can lead to several adverse health outcomes. A recent paper reviewed the scientific evidence that low ultraviolet-B exposure and vitamin D concentrations is associated with increased risk for several adverse health conditions and diseases common in this population. This paper reviews the evidence from clinical studies on the effect of vitamin D in treating these conditions and diseases for general populations. Included are asthma, autism, cancer, depression, diabetes mellitus type 2, falls and fractures, oral health, pain and sleep, and sarcopenia. Although beneficial effects have been reported for all these conditions or diseases, the patients were not completely cured. Thus, though vitamin D treatment should be considered useful and can augment standard medical practice, it generally does not replace medical treatment. It is recommended that vitamin D levels be raised to 75-125 nmol/L.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592
KEY WORDS: ■ INTELLECTUAL DISABILITIES ■ DEVELOPMENTAL DISABILITIES ■ VITAMIN D
Introduction
People with intellectual and/or developmental disabilities often have any of several adverse health conditions and diseases. Such ailments are due in part to largely staying indoors, having poor diets, and having limited physical activity. A recent paper outlined vitamin D’s role in reducing the risk of the risk of these conditions and diseases1. It was recommended that those with such disabilities try to raise 25-hydroxyvitamin D [25(OH)D] concentrations to the range of 30-50 ng/mL (75-125 nmol/L).
To achieve these concentrations could take 10005000 IU/d vitamin D3. This recommendation was in line with those from several other groups, including the U.S. Endocrine Society2 and a group of vitamin D experts who met in Warsaw in October 20123.
The present paper reviews the role vitamin D might play in treating the adverse health conditions or diseases of people with disabilities. However, unless the intended use of vitamin D treatment is for the conditions or diseases considered directly related to disability, such as autism, the information should in general also apply to those without disabilities.
Method and materials
This work is a narrative review. Pubmed.gov was searched for papers on seasonal exacerbations and treatment with vitamin D of the conditions and diseases listed in the earlier review. The search terms included vitamin D, treatment, trial, seasonal, and exacerbation, as well as the names of the conditions and diseases4. In general, this work includes only papers reporting beneficial effects of vitamin D supplementation.
Results
Asthma
Reasonable evidence exists that vitamin D reduces the severity of asthma among children but not among adults.A study involving 85 asthmatic children aged 2-14 years and 85 controls living in Turkey found that the asthmatic children had vitamin D concentrations (mean ± standard deviation) of 16.6±8.5 ng/mL, whereas the controls had concentrations of 28.2±19.5 ng/mL5. The asthmatic children also had a greater frequency of respiratory tract infections leading to emergency unit and hospital admissions. The severity of asthma was inversely correlated with 25(OH)D concentration. A review of five trials involving children given 500-2000 IU/d vitamin D3 found a significant reduction (relative risk, 0.41, 95% confidence interval, 0.27-0.63) in asthma exacerbations with vitamin D therapy6. The mechanisms whereby vitamin D reduces severity of asthma are thought to include downregulation of allergen sensitivity, enhancing steroid responsiveness, and minimizing airway inflammation7'8.
Autism
In 2008, John Cannell first proposed that vitamin D deficiency might play an important role in the etiology of autism9. He showed a strong overlap between the characteristics of autism with the effects of vitamin D deficiency as well as the effects of vitamin D sufficiency in those without autism. Cannell also suggested that vitamin D could treat the core symptoms of autism10. He noted, “Vitamin D has remarkable antioxidant, anti-inflammatory, and anti-autoimmune properties. In vitro, in vivo, and animal experiments provide compelling data for vitamin D’s role brain proliferation, differentiation, neurotrophism, neuroprotection, neurotransmission, and neuroplasticity. It also upregulates glutathione, upregulates a suite of genes involved in DNA repair and raises the seizure threshold. Adequate, perhaps pharmacological, doses of vitamin D may have a treatment effect in the core symptoms of autism.”
THESES
People with intellectual and/or developmental disabilities often have low vitamin D concentrations from staying indoors.
People with intellectual and/or developmental disabilities are prone to developing several conditions and diseases linked to low vitamin D concentrations.
Clinical studies have found that vitamin D supplementation can reduce the severity of several such conditions and diseases, including asthma, autism, cancer, depression, diabetes mellitus type 2, falls and fractures, oral health, pain, sarcopenia, and sleep
An intervention study was conducted in Egypt involving 122 children (mean age, 5.1 years) with autism. At the outset, 25(OH)D concentration was inversely correlated with Childhood Autism Rating Scale (CARS) scores (r = -0.50, p < 0.001)11. In an open trial of vitamin D3 supplementation, they received vitamin D3 (300 IU/kg/day, not to exceed 5000 IU/day) for 3 months. In the group of 16 patients that achieved 25(OH)D concentrations > 40 ng/mL, CARS scores decreased by 3.5-6.5 points. For the group of 49 patients that achieved 25(OH)D concentrations between 30 and 39 ng/mL, CARS scores decreased by 1.5-4.5 points. Those that achieved 25(OH)D concentrations < 30 ng/mL had no improvement.
A study in China involved a 32-month-old boy with autism who received vitamin D3 administered intramuscularly at a dosage of 150 000 IU every month plus 400 IU/d. This regimen raised his 25(OH)D concentration from 12.5 to 81 ng/mL12. His core symptoms of autism improved significantly after vitamin D3 supplementation.
Cancer
Strong evidence from geographical ecological studies indicates that higher solar ultraviolet-B (UVB) doses are inversely correlated with incidence and/or mortality rates for many cancers in midlatitude countries, including Australia, China, France, Japan, Spain, and the United States13. The amount of outdoor work by occupation is also inversely correlated with incidence of many cancers in Nordic countries14. These findings are considered to demonstrate the role of vitamin D in reducing cancer risk. These studies are supported by observational studies of 25(OH)D concentrations for breast and colorectal cancer15,16, as well as two randomized controlled trials of vitamin D plus calcium17, 18. Cancer survival rates have been found directly correlated with 25(OH)D concentrations for several cancers. In a study conducted in Norway, those with 25(OH)D concentrations > 81 nmol/L at time of cancer diagnosis had significantly longer 9-year survival rates than those with concentrations < 46 nmol/L for breast, lung cancer, and lymphoma, and insignificantly longer survival for colon cancer19. Better cancer survival rates for white Americans than African Americans has been attributed to the fact that African Americans have mean 25(OH)D concentrations about 40% lower than that of white Americans20. With consideration of socioeconomic status, stage at diagnosis, and treatment, the difference in survival rates for about a dozen cancers was on average about 25% higher for African Americans. That finding is consistent with the differences in mean 25(OH)D concentrations. In addition to reducing risk of cancer-specific death rates, increasing 25(OH)D concentrations after diagnosis reduces the all-cause mortality rate.
Depression
Older people with intellectual disability have a relatively high prevalence of depressive symptoms21. Several clinical trials have examined whether vitamin D can reduce the symptoms of depression. In a review published in 2014, studies were divided into those with biological flaws and those without22. The flaws were in the trial design, such as vitamin D doses that were too low or baseline 25(OH)D concentrations so high that supplementation could not further increase it. Heaney discussed such flaws23. Seven studies without biological flaws were identified and analyzed. For two of these studies, which used the Beck Depression Inventory (BDI), the average improvement was 0.78 (95% confidence interval,
24-1.27). In one of these studies24, the mean BDI for those with 25(OH)D concentration > 40 nmol/L was 4.5, whereas that for those with 25(OH)D concentration < 40 nmol/L was 6.0. For those given 40.0 IU/wk vitamin D3, BDI decreased from 4.5 to 3.0, whereas for those given 20,000 IU/wk vitamin D3, the BDI decreased from 5.0 to 4.0. Thus, although the decreases were significant, they did not eliminate depression.
Diabetes mellitus type 2
Good evidence from a meta-analysis of observational studies indicates that having 25(OH)D concentrations below 75 nmol/L increases the risk of diabetes mellitus type 225. The evidence is less clear that raising 25(OH)D concentrations after development of diabetes mellitus reduces the adverse effects of diabetes.
At least five trials have involved supplementing diabetes mellitus patients with vitamin D. A U.S. study involving obese adolescents with diabetes mellitus who were given 4000 IU/d vitamin D3 or a placebo found that vitamin D supplementation reduced fasting insulin and the Homeostasis Model Assessment-insulin resistance (HOMA-IR)26. A study involving diabetic African Americans found that vitamin D supplementation raised 25(OH)D concentration to 34 ng/mL and lowered hemoglobin A1c levels(to 7.91%)27. A study in Iran in which diabetic patients were given 4000 IU/d vitamin D3 for 2 months found a significant reduction in HbA1c (from 7.29 to 6.76%) and insulin concentration (from 8.24 to 6.55 pIU/mL), and a significant increase in high-density lipoprotein C level, but a nonsignificant decrease in HOMA-IR28.
Falls and fractures
People with disabilities are at increased risk of falls and fractures for several reasons, including largely staying indoors, low level of physical activity, poor diet, and taking pharmaceutical drugs that can reduce vitamin D levels4. To reduce the risk of falls and fractures, vitamin D supplementation of 800 IU/d is advisable on the basis of a review of vitamin D trials and fractures among older adults29. One reason for falls and fractures is impaired cognitive function, which reduces the ability to plan or react to prevent falls30. Higher vitamin D levels have been found associated with reduced risk of cognitive impairment31. Another reason for falls and fractures is weak muscles, or sarcopenia32. Vitamin D helps keep muscles strong, along with weight-bearing and resistance exercises and a diet with adequate protein33. People taking some pharmaceutical drugs, such as glucocorticoids (e.g., bisphosphonate), are at increased risk of fractures34; taking vitamin D counters this effect4.
Oral health
People with disabilities often have poor oral health, including many dental caries, missing or filled teeth, and periodontal disease. Three reasons for poor oral health include sugar intake, difficulty in cleaning teeth and massaging gums, and low 25(OH)D concentrations. Solar UVB reduces risk of dental caries and missing teeth35, as does vitamin D supplementation36. Vitamin D also reduces risk of periodontal disease37. Vitamin D maintains oral health primarily through inducing production of cathelicidin, a polypeptide with antimicrobial and antiendotoxin properties. A review in 2010 concluded: “Poor oral health in long-term care facilities has numerous causes and tragic results. Several steps, including calcium and vitamin D supplementation and careful medication monitoring can help prevent tooth loss, combat caries, and decrease periodontal disease.”38.
Pain and sleep
Children with intellectual and developmental disabilities have issues with pain and sleep that medication cannot fully address39.
A study involving older veterans with pain was conducted in a physiatry (rehabilitation) pain clinic in Atlanta, Georgia40. Before vitamin D supplementation, the mean 25(OH)D concentration was 18.6 ng/mL; after treatment with either 50,000 IU/wk vitamin D2 or 1200 IU/d vitamin D3, the concentration was 26.0 ng/mL, depending on baseline 25(OH)D concentration. After supplementation, the 10-point pain score decreased from 7.1 to 5.7, sleep duration increased from 4.6 to 5.3 hours, general health score increased by 21%, and vitality (the frequency of feeling energetic rather than feeling tired and worn out) increased by 35%. Since the increase in 25(OH)D concentration was not as high as might be desired, raising 25(OH)D concentrations higher would probably result in greater improvements. Shipton and Shipton offer a good review of the role of vitamin D in reducing pain41. Vitamin D deficiency is linked to several conditions and diseases, including headache, cancer, musculoskeletal pain, fibromyalgia, abdominal pain, ischaemia (sickle cell disease and coronary artery disease), inflammatory pain, and neuropathic pain. The review discusses several mechanisms whereby vitamin D reduces pain.
Respiratory infections
People with low 25(OH)D concentrations are at increased risk of developing respiratory infections such as influenza42. Two vitamin D randomized controlled trials found that increasing 25(OH)D concentrations by taking vitamin D reduced the risk of influenza and/or colds43'44. Although influenza is not pleasant, the primary cause of death associated with influenza is pneumonia. An ecological study found that both summertime and wintertime solar UVB doses were significantly inversely correlated with case-fatality rates in the United States associated with the 1918-1919 pandemic influenza45. Vitamin D protects against pneumonia after development of influenza in two ways: by reducing the cytokine storm, thereby protecting the linings of the lung from damage that would permit bacteria to invade, and inducing production of cathelicidin. Recent studies have also reported that low 25(OH)D concentrations are associated with increased risk of pneumonia46,47.
Sarcopenia
Vitamin D supplementation increases muscle strength. In a study conducted on women aged 50-65 years living in Brazil, increasing 25(OH)D concentration from 15 to 28 ng/mL conferred a 25% increase in muscle strength of the lower limbs. In contrast, the control group - in which 25(OH)D concentration decreased from 17 to 14 ng/mL - experienced a 7% loss in the lean mass48.
TAKE HOME MESSAGES
Raising vitamin D levels to 75-125 nmol/L can reduce the severity of several health conditions and diseases often encountered by people with intellectual and/or developmental disabilities.
Raising vitamin D levels to 75-125 nmol/L can take 10005000 IU/d vitamin D3.
Vitamin D supplements should augment, but not replace, standard medical care.
Recommendations
As discussed in the previous review4, people with developmental and/or intellectual disabilities should seek to obtain sufficient vitamin D from diet, supplements, and solar UVB to keep 25(OH)D concentrations in the range of 75-125 nmol/L. Reaching this range could take 1000-5000 IU/d vitamin D3. For people being treated for any of the conditions or diseases discussed here, somewhat higher oral vitamin D intake might be required at first since vitamin D deficiency may have preceded the development of the condition or disease. One clinical study gave loading doses of 100,000, 200,000, and 300,000 IU of vitamin D3. From the results of that study, researchers developed a nomogram to guide the dose for any desired increase in 25(OH)D concentration in terms of international units per kilogram of body weight, assuming the person had 25(OH)D concentration below 50 nmol/L. The equation found was A 25(OH)D =0.025! (dose per kg body weight)49. After that one-time dose, a dose of 1000-5000 IU/d can be given. Although not the subject of this review, other changes in lifestyle would improve quality of life for people with intellectual and/or developmental disabilities. Such changes include a healthy diet, keeping weight down, and regular physical activity. A recent paper outlines nutrition services guidelines for this group50. ■
[Vitamin D in dermatologists' practice] English abstract
Jarosław Bogaczewicz
Katedra i Klinika Dermatologii i Wenerologii Uniwersytetu Medycznego w Łodzi
The use of vitamin D in a daily practice of dermatologist is not limited to the topical treatment of skin diseases, particularly psoriasis. The risk of vitamin D deficiency in patients with photosensitivity, which require photoprotection because of primary photodermatoses, such as solar urticaria, polymorphous light eruption, actinic prurigo, chronic actinic dermatitis, and also in secondary photodermatoses, which are manifestation of systemic diseases, including porphyrias, pemphigus, dermatomyositis, and systemic lupus erythematosus justifies the usage of oral supplementation with vitamin D. The next group of patients with the justified supplementation includes patients undergoing long-term glucocorticoid therapy because of autoimmune blistering skin diseases and autoimmune connective tissue diseases, primary systemic vasculitis, and pyoderma gangrenosum. The knowledge of mechanisms responsible for vitamin D action, and also metabolic consequences of its deficiency, makes possible the wide usage of both vitamin D and its analogues in a daily practice of dermatologist. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 112-116 KEY WORDS: ■ VITAMIN D ■ CALCITRIOL ■ CALCIPOTRIOL ■ TACALCITOL ■ SKIN
The role of VDR gene polymorphisms in basal cell carcinoma development
Aleksandra Lesiak
Department of Dermatology, Medical University of Lodz
Basal cell carcinomas (BCC) are the most common cancers in Caucasian population. Their pathogenesis is not fully known, however genetic and environmental factors are relevant. Among genetic disturbances, genes encoding intracellular signaling pathways and regulatory proteins are considered as the most important. In recent years the associations between polymorphisms in VDR gene and different internal organs and skin neoplasms were found. The aim of the study was to assess the frequency of four polymorphisms in the VDR gene (Fokl, Bsml, Taql and Apal) in 142 patients of Polish origin with BCC and the same number of controls. The expression of VDR protein in the skin and the vitamin D status in a subset of patients and controls were also measured. The polymorphisms were assayed by PCR-RFLP, the VDR proteins by Western blot and 25(OH)D serum level by RIA.
Results: The presence of TT genotype in Fokl VDR polymorphism resulted in over 10-fold higher risk for BCC development. VDR expression was significantly higher in BCC patients than in the control group (p < 0.01). Median serum level of 25(OH)D was significantly higher in the control group when compared to BCC patients (p=0.0026). VDR gene polymorphisms are involved in basal cell carcinoma development in the patiens of Polish orgin. Currently published data on vitamin D status in BCC are ecquivocal and require further complex studies. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592 KEY WORDS: ■ BASAL CELL CARCINOMA ■ VDR GEN POLYMORPHISM ■ CANCEROGENESIS
Introduction
Basal cell carcinomas (BCCs) are the most common skin tumors in Caucasians. According to American database, approximately 1000000 new cancers develop per year and the number continuously increases each year1. In Poland there is a lack of statistical data concerning the prevalence of BCC but regional data from the north of the country indicate a recent increase in the incidence rate1. In most European countries, BCCs are not included in national cancer registries so an accurate picture of BCC prevalence and any change in incidence over time is difficult to obtain. Although BCCs are rarely life-threatening, they pose financial impact1,2. The main risk factor for BCCs is extensive exposure to ultraviolet radiation, especially UVB, which simultaneously cause DNA damage in keratinocytes and vitamin D synthesis by the same cells. This observation led to formation of hypothesis that vitamin D formation in the epidermis may be an innate protective mechanism against UV damage3.
Genetic background of BCC includes multiple genes like sonic hedgehog pathway genes, mainly PTCH1 and GLI- 1 and-2, gene encoding vitamin D receptor (VDR) and gene encoding methylenetetra- hydrofolate reductase (MTHFR), which is critical in folate metabolism and DNA repair4-6. The VDR gene is located on chromosome 12ql2-ql4. The most frequently occuring VDR polymorphisms which were described to be associated with cancerogene- sis are FokI (rs2228570), BsmI (rs1544410), Apal (rs7975232) and TaqI (rs731236). VDR is responsible for cellular effects of vitamin D, regulation of various intaracellural signaling pathways which are involved in cancerogenesis7-9. Genetic polymorphisms in VDR influence the level of vitamin D synthesis in the skin, liver and kidney, its metabolism and degradation. VDR is expressed on kerati- nocytes and is a natural ligand for calcitriol which has the ability to inhibit proliferation, induces differentiation of human keratinocytes and modulates activity of over 60 genes10-12. Increased VDR expression was found in various cancer cells, including skin tumors like squamous cell carcinoma, basal cell carcinoma and melanoma however the results are equivocal and somewhat contradictory13.
Material and Methods
The study group consisted of 142 BCC patients who were diagnosed in Department of Dermatology Medical University of Lodz, between 2005-2008. They were all Caucasian (71 M, 71 F, mean age 56 years old, range 45-78 years) and none was an organ transplant recipient, was being treated with immunosuppressive drugs or suffered from any other malignancy. BCC was diagnosed based on histological findings. The patients were recruited at first attendance and skin biopsies for Western blot analysis and blood samples were taken at the second visit when diagnosis was confirmed (approx. 2 weeks after the first visit). Only the patiens with nodular BCC located on the area of upper cheek were included into the study. Additionaly 142 age and sex matched healthy subjects were enrolled into the sudy and served as a control group. Each subject gave written informed consent before entering the study which had been approved by the local Ethics Committee. Blood samples for DNA genotyping were taken among all subjects. Moreover in 79 BCC (mean age 60.2 years old, 41F, 38 M, phototype: I/II-20, III-52, IV-7) patients and in 46 control subjects (mean age 58.4 years old, 21F, 25 M, phototype: I/II-10, III-28, IV-8) serum samples were taken for analysis of 25(OH)D level. Additionally skin specimens were taken from lesional skin in 44 BCC (mean age 59.2 years old, 20F, 24 M, phototype: I/II-10,
THESES
We selected candidate polymorphisms in VDR gene (FokI, BsmI, TaqI and Apal in the VDR gene) which have been reported to be associated with altered function of the encoded proteins or cancer risks in earlier epidemiologic studies. We assessed them in relation to BCC risk in Polish population.
We examined the expression of VDR protein in BCC in comparison with their expression in normal healthy skin.
Despite some evidence that vitamin D and its receptor are involved in cutaneous carcinogenesis there is lack of data on vitamin D status among BCC patiens, thus we also decided to dertermine serum level of 25(OH)D.
To our knowledge, there have been no similar studies performed in Eastern European Caucasian population of BCC patients by now and our study is the first one.
Statistical methods
The chi-squared tests were used to detect a significant deviation in genotype frequency from Hardy- Weinberg equilibrium. The associations between different dychotomic variables and independent variables were assessed by logistic regression analysis. The allelic frequencies were estimated by gene counting and genotypes were scored. The odds ratio (OR) and 95% confidence intervals (Cl) were calculated with the use of the logistic regression model. STATISTICA 6.0 Software (Statsoft, Tulsa, OK, USA) was employed to perform analyses. P values lower than 0.05 were considered as statistically significant.
Results
The genotype distributions of all the analysed polymorphisms were in Hardy-Weinberg equilibrium. The genotype distribution for Apal, FokI and TaqI polymorphisms in the VDR gene differed statistically between BCC patients and the controls while no sta- stistically significant difference was found for BsmI polymorphism. Analysis of genotypes distribution for each of the examined polymorphisms is presented in Table 2. In multivariate regression analysis we found that TT genotype in FokI polymorphism significantly increased the risk for BCC development (OR=10.14, p<0.001) and this association was the strongest one. Other genotypes such as GT in ApaI and TT and TC in TaqI also significantly increased the risk for BCC, although calculated relative risk for these associations were lower (Table 3). Additionally we found no correlation between analysed polymorphisms in the VDR gene and constitutional features such as eye and hair colour and skin phototype (p>0.05 for all comparisons). Allele T in FokI, allele T in Apal and allele C in TaqI polymorphisms were noted more frequently among BCC patients than in healthy subjects (p<0.001 for all comparisons). All analysed biopsies revealed VDR expression. VDR expression was significantly higher in BCC patients than in the control group (median 1.4x106 IDV vs. median 0.4x106 IDV; p < 0.001). Analysing level of expression of VDR together with their polymorphisms we found that BCC patients who have CC genotype in Taq I polymorphism have significantly higher expression of VDR (median 1.7x106 IDV) when compared to TT carriers (median 1.3x106 IDV) p<0.05. Similar analysis was performed for FokI, Bsm I and Apal but no statistical correlations were observed (p > 0.05 for all comparisons).
Median serum level of 25(OH)D was significantly higher in the control group when compared to BCC patients (29.5 ng/ml vs. 24. 2 ng/ml; p=0.0026). 28 (35.4%) subjects out of all 79 analysed BCC patients, had vitamin D serum level below 20 ng/ml while other 30 (38%) patients had vitamin D level between 20-30 ng/ml, in other subjects (n=21; 26.6%) 25(OH)D serum level was above 30 ng/ml. Contrary, only 5 (10.9%) subjects from control group has vitamin D level below 20ng/ml, and 20 (43.5%) between 20-30 ng/ml and 21 subject (45.5%) over 30ng/ml.
Discusion
Vitamin D receptor is expressed on various mali- gnat cells including basal cell carcinoma and squ- amosus cell carcinoama. Main functional targets of this receptor are mineral metabolism, but also regulation of many metabolic pathways, such as those involved in the immune response and cancer3. In recent years, the relevance of VDR polymorphisms for various types of cancer has been investigated by a great number of studies. It has been hypothesized that VDR polymorphisms may influence both the risk of cancer occurrence and prognosis. To date, the results of the studies investigating the associations between specific VDR polymorphisms and cancer are not consistent. There are scarce data on the association between VDR polymorphisms and non-melanoma skin cancers (NMSC). Gandini et al. performed metaanlysis with a total of 6805 skin cancer cases in regard to two polymorphisms FokI and BsmI and vitamin D intake. They showed correlation between melanoma and NMSC and two of the analysed polymorphisms with the relative risk being approximately. In our study the presence of TT genotype in FokI polymorphism caused over 10-fold risk for BCC development. Other genotypes such as GT in ApaI and TT and TC in TaqI were also statistically linked with cancer, however the calculated risk ratio was lower. These observations are in line with the results obtained by Han et al.5. Similarly to other authors we found no correlation between BCC and BsmI polymorphism5'14. The risk ratio for TT FokI polymorphism obtained in our statistical analysis was much higher than in the presented meta-analysis by Gandini et al.14. These results should be proven by the study on the larger population, however, currently we may point out to TT genotype in FokI polymorphism as one of the risk factors for BCC in Polish population. Reichrath et al. showed that VDR staining intensity and expression for VDR mRNA is much stronger in biopsies taken from BCCs than from adjacent tumor skin or normal human skin. The authors suggested that strong expression of VDR may be involved in the growth regulation of BCC. In our study the results are similar as we found a significantly increase in VDR expression in the BCC biopsies. To date it is still unclear whether its increased expression in the cancer tissue is linked with the BCC capacity to synthesize calcitriol from vitamin D. We suggest that it may be linked with the presence of VDR polymorphisms in BCC patients which cause formation of at least partially inactive protein with no ability to bind with its ligand. The enhanced VDR expression perhaps is a protective mechanism of the human organism. This mechanism of feedback loop is suggested by Reicharth et al.15. Although in our study VDR expression was much higher in BCC than in normal skin, the lowest intensity was found in the patients with TT TaqI polymorphism which gave over 3-fold risk for BCC development. This phenomenon needs further studies and currently is difficult to be explained. Similar observations on enhanced expression of VDR concern squamous cell carcinoma16, however VDR staining did not corralate with histological type of SCC, grading or markers of proliferation17,18. Recently published data by Asgari et al.19 showed the association between increased risk for BCC development and higher prediagnostic serum concentration of 25(OH)D. In the light of the fact there are no available data comparing serum 25(OH)D levels in a population-based sample of individuals with BCC to controls, this observation seems to be very interesting and the staus of vitamin D in BCC patiens should be the subject for further studies. In contrast, studies conducted in vitro revealed that high level of vitamine D caused inhibition of BCC growth20.
In our study we examined 25(OH)D serum level as it reflects its internal status and is considered superior to measures of vitamin D intake by dietary questionaires alone or predictors of vitamin D status. Moreover according to literature data, this metabolite is a valid measure of vitamin D level within even several months21. In published data no association between dietary intake of vitamin D and BCC risk has been found14,22.
We found that 25(OH)D serum level was significantly lower in BCC patients than in matched control, however in majority of the subjects from both groups 25(OH) D level was below 30 ng/ml. Our observation on the lower vitamin D level in both groups should be carefully interpreted as it is widely known that in older adults
TAKE HOME MESSAGES
Obtained results testify for importance of VDR polymorphisms in skin cancerogenesis.
Enhanced expression of VDR in skin biopsies taken from BCC lesions indicates the role of these VDR pathways in the pathogenesis of basal cell carcinoma.
Lower Vitamin D concentration in BCC when compared to the controls may suggest impaired vitamine D system regarded as importat immunomodulator involved in various physiological and pathological pathways
Vitamin D and melanoma
Anna A. Brożyna
Department of Tumor Pathology and Pathomorphology, Oncology Centre - Prof. Franciszek Łukaszczyk Memorial Hospital, the Ludwik Rydygier Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń
Cutaneous melanoma is one of the most rapidly increasing malignancy worldwide and represents a significant burden to society and public health, especially in Caucasians. Since the most efficient treatment mode, surgical removal, is limited to the localized disease, there is a need for new treatment modalities of metastatic disease. Vitamin D and its derivatives modulate multitude important physiological processes and functions, including the cellular proliferation, differentiation, apoptosis and immunological processes and protects against oncogenesis. Recently several vitamin D derivatives, with anti-melanoma activity in vitro, have been identified. The low serum level of vitamin D in melanoma patients is associated with more advanced tumor and poorer prognosis. Vitamin D exerts its effects acting via specific nuclear receptor (vitamin D receptor, VDR), expressed in intestine, bone and other tissues, including skin. The disturbances and/or reduction in VDR expression and CYP27B1, the enzyme required for activation of vitamin D, is observed in melanoma cells and lack or low VDR and CYP27B1 immunoreactivity is related to stage of melanoma progression, the presence of markers of poor prognosis and shorter overall and disease-free survival of melanoma patients. In addition, CYP24A1 expression decreases during melanoma progression being the lowest in advanced melanoma stages and metastases. Furthermore, CYP24A1 expression negatively correlates to the presence of markers of poor prognosis and positively correlates with overall and disease-free survival. Thus it is proposed the use of vitamin D as an adjuvant or main therapeutic agent in melanoma treatment. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592 KEY WORDS: ■ CUTANEOUS MELANOMA ■ VITAMIN D ■ VITAMIN D DERIVATIVES ■ CYP27B1 ■ VDR ■ CYP24A1
Cutaneous melanoma, growing problem in health
Cutaneous melanoma became a common malignancy worldwide and represents a significant burden to society and public health, especially in whites. Melanoma incidence has been increasing during the last few decades with annual increase of incidence ranging from 3% to 7% in white population, especially in older population1,2. In recent years new therapeutic agents, related to immune response and targeted mutated molecular pathways, have been approved for the treatment of metastatic melanoma. Regardless of promising effects on disease free and overall survival, the high costs of treatment and undesirable side effects make these therapies limited, thus survival is slightly improved, but still is unsatisfactory P The most efficient treatment mode is surgical excision, but it is limited to the localized disease (stage I and II), and for metastatic melanomas there is still no reliable therapy3-6. Therefore there is a need to develop new strategies in treatment of advanced melanomas.
Vitamin D insufficiency and melanoma
Vitamin D comprises a group of fat-soluble seco- steroids, which are represented by the two major forms: vitamin D2 and vitamin D3. Vitamin D3 is absorbed from the diet or made in the skin from 7-dehydrocholesterol after UVB-induced photoconversion7'8. Both vitamin D from the food and cutaneous synthesis are considered biologically inactive until it undergoes two sequential enzymatic hydroxylation, in the liver to 25-hydroxyvitamin D3 (25(OH)D3) by CYP2R1 and/or CYP27A1, and in the kidney to 1,25-dihydroxyvitamin D (1,25(OH)2D3) by CYP27B19-12. It has been also shown that skin cells including keratinocytes, macrophages, melanocytes and various other normal and cancerous cell types express the enzymes essential to produce 1,25(OH)2D313-17. In addition to the classic role of vitamin D related to maintaining the calcium and phosphate homeostasis, its biologically active form exerts pleiotropic effects on various organs and tissues. For the last several years, serum 25-hy- droxyvitamin D deficiency has been linked to increased risk of various cancers7,8,18. Similarly, vitamin D is also crucial in cutaneous melanoma outcome. Recent published data reveals that higher 25-hy- droxyvitamin D3 level is associated with lower Breslow thickness at diagnosis19. Furthermore, lower vitamin D level is also related to melanoma ulceration (marker of poor prognosis), shorter overall survival and increased risk for melanoma-specific death20,21.
**Vitamin D as melanoma cells growth inhibitor))
As has been shown in in vitro and in vivo in animal studies, apart from regulating calcium and phosphate homeostasis, 1,25(OH)2D3 exerts anti-proliferative and pro-differentiating effects on a wide range of normal and cancerous cell types. The first showing inhibitory effect of 1,25(OH)2D3 on melanoma cells was published more than 30 years ago22. Subsequent experiment confirmed anti-cancer properties of 1,25(OH)2D3[reviewed in23]. Unfortunately, the use of high doses of calcitriol for cancer treatment is limited due to its hypercalcemic effects. Thus new vitamin D derivatives have been developed and identified to minimize the calcemic side effects while preserving anticancer properties of calcitriol.* THESES *1. Cutaneous melanoma incidence has been increasing during the last few decades and melanoma is responsible for most skin cancer deaths (account for 80% of deaths from skin cancer). The prognosis for patients with metastatic melanoma remains poor due to low efficiency of existing adjuvant therapies.
In addition to maintaining calcium homeostasis and to promotion of the bone health, normal serum vitamin D levels, proper vitamin D metabolism and vitamin D signaling may play a role in prevention or therapy of cancer.
Skin cells activate vitamin D via classical and non-classical pathways, producing vitamin D analogs with pro-differentiation, anti-proliferative and anti-cancer properties.
Furthermore, new pathway of vitamin D metabolism has been discovered that use alternative activating enzymes24-27. These alternative pathways operate in vivo28-30 and generate novel analogs as 20-hydroxyvitamin D3/2, 20,23(OH)2D, 1,20(OH)2D3, 20,24(OH)2D3and20,25(OH)2D3, with potent anti-proliferative and pro-differentiation activities in normal and malignant cells, including melanoma cells31-34. These analogs also use alternative nuclear receptors to VDR35.* Disturbances of vitamin D signaling in melanoma *1,25(OH)2D3 exerts its biological effects via binding to a specific nuclear receptor (vitamin D receptor, VDR), that belongs to the superfamily of steroid nuclear receptors. VDR is expressed in almost all tissues and cells including skin7,8. Thus the skin cells are able to synthesize the biologically active vitamin D and to response to growth and differentiation regulatory action of calcitriol. Growing evidence suggests that invalid vitamin D activation and signaling disturb physiological effects of calcitriol and its protection against cancer. The reduction in VDR expression is observed in melanoma cells and is related to melanoma progression and being observed in more advanced tumors (higher: Breslow thickness, higher Clark level and stage). The presence of markers of poor melanoma prognosis (higher mitotic index, nodular type, ulceration and lack or non-brisk tumor infiltrating lymphocytes (TILs)) and shorter overall and disease-free survival are accompanied by lower VDR expression36,37. Also VDR gene polymorphisms can alter susceptibility and prognosis of patients with melanoma [reviewed in23]. Similarly, significantly reduced expression of CYP2B1 is observed in melanomas showing more malignant phenotype (vertical growth phase, higher Clark levels and Breslow thickness, metastasizing).
Lack or low CYP27B1 level is also related to poorer prognosis, as assesses by shorter overall and disease-free survival of melanoma patients38. CYP24A1 levels decreased during melanoma progression being the lowest in advanced stages and metastases. CYP24A1 expression negatively correlates to the presence of markers of worse prognosis and positively correlates with overall and disease-free survival39. The best known role of CYP24A1 is inactivating cal- citriol. These unexpected pattern of CYP24A1 immu- nostaining in human melanomas could in part be explained by the recent discovery that CYP24A1 generates also active vitamin D hydroxyderivatives, showing anti-cancer properties34. Thus in addition to systemic, local vitamin D endocrine system affects melanoma behavior and appears to have an important impact on the formation of melanocytic nevi and melanomagenesis, or progression, at early stages of tumor development. ■
Acknowledgements: Writing of this paper was supported in part by grant 2014/15/B/NZ4/00751 from National Science Centre, Poland. Author wish to thank Professor Andrzej T. Słomiński for his support in studies and writing this paper.* TAKE HOME MESSAGES *1. Melanoma development and progression related to shorter overall survival and disease-free survival time appear to be linked with disturbances in vitamin D metabolism and defects in vitamin D signaling in melanoma cells. The evaluation of VDR and CYP27B1 expression could also have important implications for the diagnosis and for predicting clinical outcome.
Low serum level of vitamin D in melanoma patients is associated with more advanced tumor and poorer prognosis.
Vitamin D, showing antitumor activities against melanoma cells, represents promising adjuvant therapeutic in melanoma treatment.
Potential use of vitamin D analogs in the treatment of skin diseases
Michał A. Żmijewski
Katedra Histologii, Gdański Uniwersytet Medyczny
Human skin is not only a natural source of vitamin D, but also place of its metabolism and immediate aim of its biological activities. Under physiological conditions, vitamin D regulates proliferation and differentiation of keratinocytes, thus is involved in the regulation of the renewal of epidermal barrier. Moreover, vitamin D modulates the immune response in the skin. Given the multidirectional activities of vitamin D in the skin, it should not be surprising that reduced level of vitamin D in the body, caused by improper supplementation, or by specific genetics background affects development or worsen the symptoms of many skin diseases. Thus, vitamin D and its analogs are increasingly used in the treatment of skin diseases; typically as a part of a combination therapy. It should be emphasized that vitamin D analogs such as: commonly used in psoriasis calcipotriol or analog recently tested 20-hydroxyvitamin D do not affect the calcium and phosphate levels and can therefore be safely used in the therapy. In addition to psoriasis, the vitamin D analogs are currently extensively investigated in the treatment of atopic dermatitis, vitiligo, or skin lesions associated with scleroderma. Furthermore, vitamin D analogs can be successfully used directly on the skin as an ointment. Great hope is also associated with the use of vitamin D and its analogs in the treatment of skin cancers, including the most dangerous of them melanoma. A series of laboratory tests, preclinical and clinical studies indicated that these compounds inhibit growth of cancer cells. It should be noted that, maintaining optimal level of vitamin D (30-50 ng/mL in serum) reduces the probability of development of skin diseases, including cancer and improves treatment. It should be emphasized that the best source of vitamin D is our skin exposed to the sunlight, but extensive exposure to ultraviolet radiation, may lead to skin cancer and therefore supplementation should be considered. In conclusion, vitamin D plays a key role in the physiology of the skin in human, and its deficiency is observed in multiple skin diseases. Thus, vitamin D should be an important element in the prevention and treatment of skin diseases, including cancer.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 112-116
KEY WORDS: ■ VITAMIN D ■ VITAMIN D ANALOGUES ■ KERATINOCYTES ■ PSORIASIS ■ SKIN CANCER
Biomarkers of Vitamin D Metabolism: Current State of Knowledge
Glenville Jones
Department of Biomedical & Molecular Sciences, Queen's University, Kingston Ontario, Canada
Vitamin D metabolism is complex and features multiple metabolites, many still without clear biological functions.These vitamin D metabolites are synthesized by a set of specific cytochrome P450 enzymes, gene deletion of which have helped us to understand which vitamin D metabolites are the most important. The central pathway involves the main circulating metabolite, 25(OH)D3 made by CYP2R1 and the hormonal form, 1,25(OH)2D3 produced by CYP27B1. Mutations of these two enzymes result in rickets. 25(OH)D3 and 1,25(OH)2D3 remain the principal biomarkers of vitamin D; 25(OH)D3 as an indicator of vitamin D supply and 1,25(OH)2D3 as an indicator of biological action. Another emerging biomarker is 24,25(OH)2D3, made by the catabolic CYP24A1, which is an indicator of vitamin D degradation. Mutations of CYP24A1 result in hypercalcemia. All three of these biomarkers can be assayed in serum/plasma by either a combination of antibody-based assays or simultaneously by LCMS/MS. A variety of other vitamin D metabolites can be measured but have limited usefulness because of unknown function. These include: vitamin D3 itself, 3-epi-25(OH)D3, 25,26(OH)2D3, 25(OH)D3-26,23-lactone, 1,24,25(OH)3D3. Recently, there has been a resurgence of interest in assaying the levels of bioavailable or free 25(OH)D3 and free 1,25(OH)2D3 as measures of the amount of steroid unbound to the plasma proteins, DBP or albumin and available to enter cells and produce biological effects. The utility of each of these biomarkers will be discussed. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592 KEY WORDS: ■ 25(OH)D3,1,25(OH)2D3, 24,25(OH)2D3
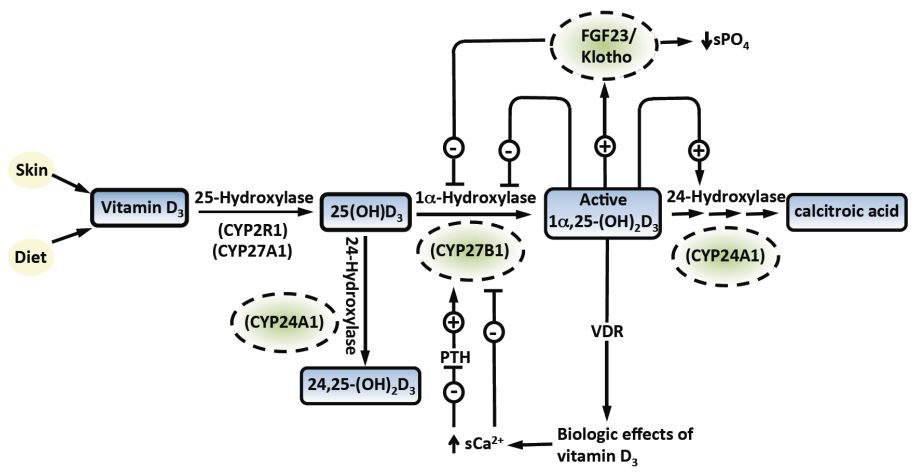
Introduction
Vitamin D3 is metabolized, firstly in the liver by CYP2R1 [vitamin D3-25-hydroxylase] to 25(OH)D3; then by CYP27B1 [25(OH)D3-1a-hydroxylase], primarily in the kidney, to the active form, 1,25(OH)2D3 (Figure 1)1. The hormone modulates transcription of a number of genes, particularly those involved in calcium and phosphate homeostasis; as well as some genes involved in non-calcemic functions, such as in promotion of cell differentiation and inhibition of cell proliferation2. Genetic mutations of either CYP2R1 or CYP27B1 result in low levels or the absence of 25(OH)D3 or 1,25(OH)2D3 respectively and causing rickets1. Thus, it is easy to see why the serum levels of the precursor, 25(OH)D3 or the serum levels of the hormone, 1,25(OH)2D3 might be biomarkers for vitamin D supply or biological action respectively.
Since the cloning of CYP27B1 and the demonstration that this enzyme is found in many extra-renal sites around the body, the viewpoint has prevailed that the enzyme is there to synthesize l,25(OH)2D3 locally and augment the renal production3. Should this hypothesis be correct then the serum 25(OH)D3 assumes a much greater importance, as it dictates the extrarenal synthesis of l,25(OH)2D3 which has been described as not subject to the same kind of tight regulation as that found in the kidney. Indeed, serum 25(OH)D3 has become a surrogate biomarker for tissue l,25(OH)2D3 since there are many studies which show that levels of 25(OH)2D3 associate with multiple clinical outcomes from cancer prevention to cardiovascular health4.
Accordingly, serum 25(OH)D3 is considered by some researchers to be a biomarker of biological action, particularly in non-calcemic functions of vitamin D4. The identification of idiopathic infantile hypercalcemia (IIH) patients with mutations of the catabolic cytochrome P450, CYP24A1 [25(OH)D3-24-hydroxylase]5 has stimulated the search for suitable biomarker for the disease. The obvious candidate, serum 24,25(OH)2D3 should be low or undetectable in this disease but this is also the case in vitamin D deficiency. Consequently, we have suggested that a more reliable biomarker for IIH due to loss-of-function CYP24A1 mutations is the ratio of 25(OH)D3:24,25(OH)2D3 which is in the range of 5-25 in normal individuals, rises slightly in vitamin D deficiency and exceeds 80 in IIH patients6.
Dogma has prevailed for decades that, as with other steroid hormones, 1,25(OH)2D3 works in target cells by dissociating from DBP and other plasma proteins; free ligand diffusing into the cell; and interacting with the VDR to change rates of gene transcription inside the nucleus2. This has generated a great deal of interest in measuring or calculating the bioavailable or free 1,25(OH)2D3 concentrations inside target cells either experimentally or indirectly by measuring total 1,25(OH)2D3 and DBP levels and by calculating the free ligand value from knowledge of affinity of DBP for the ligand7,8. Similarly free 25(OH)D3 can also be targeted using similar techniques9. Recent well-publicized attempts to measure free 25(OH)D3 concentrations in Afro-Americans as compared to Caucasians have been discredited because of the use of a defective antibody that does not detect all genetic forms of DBP equally10,11. Consequently, most experts in the field believe that the value of measuring free 25(OH)D3 or free 1,25(OH)2D3 as biomarkers has yet to be proven.
Many other vitamin D metabolites have been identified in human serum over the past four decades, but most, if not all, of these compounds are of unknown function or are considered to be inactive because they do not bind with strong affinity to VDR or have minimal biological activity in vivo. These include vitamin D3 itself, 3-epi-25(OH)D3, 25,26(OH)2D3, 25(OH)D3-26,23-lactone and 1,24,25(OH)3D3. As a result, these metabolites are unlikely to ever be classified as biomarkers of vitamin D. Perhaps the most obvious candidate for biomarker of vitamin D action should be the tissue concentration of 1,25(OH)2D312. LC-MS/MS techniques for studying the picomolar or femtomolar concentrations of 1,25(OH)2D3 expected in target tissues are approaching the sensitivity required for this difficult problem. But study of this parameter is also hampered by the lack of availability of biopsied target tissue. Thus, we are some way away from having a direct biomarker of vitamin D action inside target cells.* Assays used for Measurement of Biomarkers *25(OH)D
These methods are designed to measure the 25-hydroxylated metabolites of both vitamin D3 and vitamin D2 and thus report either the two parameters combined as total 25(OH)D which is the clinically relevant parameter or the two separate 25(OH)D2 and 25(OH)D3 values that must be summed together. Currently, the most popular methods involve antibody-based immunoassays and liquid-chromatography-mass spectrometry (LC-MS/MS)-based assays13. Immunoassays are non-chromatographic, usually automated and dependent upon the specificity of the antibodies used for their ability to measure 25(OH) D3 & 25(OH)D2 equally well and exclude interferences such as 24,25(OH)2D3. LC-MS/MS requires expensive instrumentation; uses chromatography and assay several vitamin D metabolites simultaneously based upon their molecular mass. LC-MS/ MS methods are superior to immunoassays in terms of assay performance in terms of accuracy, coefficient of variability, as judged by quality assurance schemes such as DEQAS and the VDSP [discussed in sections following;14,15]. NIST provides reference standards for 25(OH)D assay and also contributes to the DEQAS program by supplying reference values for circulated samples.
1,25(OH)2D
Current assays involve antibody-based immunoassays which are non-chromatographic, automated and use antibodies that detect both 1,25(OH)2D3 and 1,25(OH)2D2. Methods based upon liquid-chromatography-mass spectrometry (LC-MS/MS) approaches are still in their infancy and usually employ preparatory steps involving immuno-purification to remove other dihydroxyvitamin D metabolites present in serum at 100-1000 times the level of 1,25(OH)2D and derivatization in order to achieve the detection of pmol/L of steroid16. DEQAS runs an external assessment scheme for 1,25(OH)2D with results based upon the all-laboratory trimmed mean (ALTM).
24,25(OH)2D3
The previous generation of methods for measuring 24,25(OH)2D3 used a competitive protein-binding assay approach based upon binding to DBP, which has an equal affinity for 25(OH)D3 and 24,25(OH)2D3, and thus the assay required a step of chromatography to separate the two metabolites17. A more modern approach is to use LC-MS/MS to assay 24,25(OH)2D3 using a detection based upon its molecular mass. 24,25(OH)2D3 is the most abundant of the dihydroxyvitamin D metabolites, its normal level exceeding that of 1,25(OH)2D3 by two orders of magnitude. In reality, these two dihydroxyvitamin D metabolites are resolved on the LC step. NIST is currently developing a LC-MS/MS-based reference method and reference standards for 24,25(OH)2D3 determination. It should be noted that LC-MS/ MS permits the simultaneous assay of 25(OH)D3, 25(OH)D2 and 24,25(OH)2D3. This allows for the determination of the ratio of 25(OH)D3:24,25(OH)2D3 which some researchers believe is a more useful parameter than the 24,25(OH)2D3 alone6,18.* Application of Biomarkers of Vitamin Metabolism *Serum 25(OH)D
This biomarker of vitamin D status has found widespread use as an indicator of vitamin D deficiency, vitamin D sufficiency and vitamin D toxicity. The Institute of Medicine (IOM) Report 2011 defined these ranges of serum 25(OH)D as 0-50 nmol/L; 50-125 nmol/L; and above 125 nmol/L respectively13. Based upon published evidence, IOM stated that clinical symptoms of vitamin D deficiency are observed at levels below 30 nmol/L. The Endocrine Society has published guidelines that claim that vitamin D insufficiency includes individuals with <75 nmol/L19. Acute vitamin D toxicity as is observed in hypervitaminosis D requires doses of vitamin D3 >10,000 IU/day and possible even higher depending upon the duration of the exposure20. In clinical chemistry terms, this corresponds to a serum 25(OH)D value of 400- 500 nmol/L.
Some evidence from epidemiological studies suggests that serum 25(OH)D levels between 125-400 nmol/L resulting from chronic high dosing with vitamin D at > 4000 IU/day results in higher risk of some forms of cancer and higher mortality13.
In recent years serum 25(OH)D has also become a surrogate biomarker for vitamin D action in its putative non-calcemic or pleiotropic effects3'4. Many epidemiological studies have noted that low serum 25(OH)D associates with a number of deleterious health outcomes. It is hypothesized that these associations are the result of serum 25(OH)D being correlated with target cell 25(OH)D' which acts as substrate for the extra-renal CYP27B1' and in turn correlates with target cell 1'25(OH)2D levels. In this way' serum 25(OH)D is an easily-measurable surrogate for intracellular 1'25(OH)2D concentrations inside extra-renal target cells.
Serum 1,25(OH)2D
This biomarker of vitamin D action is used only sparingly by endocrinologists to differentiate between various hypocalcemic and hypercalcemic conditions21. It is most useful in diagnosing sarcoidosis' that is caused by uncontrolled CYP27B1 activity in sarcoid tissue resulting in elevated 1'25(OH)2D levels. Serum 1'25(OH)2D levels do not correlate with vitamin D outcomes in part because the hormone has a short t% in the bloodstream and possibly because it is also produced extra-renally for some of its putative effects.
Serum 24,25(OH)2D3 or Ratio of 25(OH)D3:24,25(OH)2D3
This biomarker of vitamin D degradation has only recently come back into favour after three decades of being ignored. Loss-of-function mutations of CY- P24A1 result in very low 24'25(OH)2D3 levels and elevated 25(OH)D3:24'25(OH)2D3 ratios5'6'22. This has become a useful screening tool for hypercalcemic patients suspected of having IIH due to CYP24A1 mutations prior to expensive genetic testing22. The 25(OH)D3:24'25(OH)2D3 ratio also allows the physician to distinguish between IIH due to mutations of CYP24A1 and those due to mutations of SLC-34 (Na-Pi IIa co-transporter)23. Patients with either of these rare conditions often exhibit symptoms of nephrolithiasis or nephrocalcinosis5'17'23'24' so that there is interest currently in whether serum 24'25(OH)2D3 or the 25(OH)D3:24'25(OH)2D3 ratio might be useful biomarkers for renal stones. The invention of a convenient' sensitive and accurate assay of 24'25(OH)2D3 has allowed for the screening of large populations of individuals for the relationship between 25(OH)D3 and 24'25(OH)2D3. At low serum 25(OH)D3 values' serum 24'25(OH)2D3 is virtually undetectable suggesting that the production of 24'25(OH)2D3 by CYP24A1 is turned off6'24. This threshold seems to correspond with the threshold for vitamin D deficiency of around 30 nmol/L.* Conclusions: *1. Serum 25(OH)D3 is a proven biomarker for vitamin D supply and status. Some experts hypothesize that serum 25(OH)D3 is also a biomarker for vitamin D action inside target cells expressing extra-renal CYP27B1 and engaged in transcriptional regulation of non-calcemic genes. Consequently' serum 25(OH)D3 may serve as a surrogate for intracellular 1'25(OH)2D3
Serum 1'25(OH)2D3 is a biomarker for vitamin D action in calcium/phosphate homeostasis.
Serum 24'25(OH)2D3 or the 25(OH)D3: 24'25(OH)2D3 ratio are biomarkers of vitamin D breakdown
Simultaneously monitoring all three biomarkers using LC-MS/MS might prove to be optimal.
Standardization of Vitamin D Assays:
The past and present dilemma for vitamin D research
Christopher T. Sempos
Coordinator, Vitamin D Standardization Program (VDSP)
The serum concentration of total 25-hydroxyvitamin D [25(OH)D] is considered to be the principal clinical marker for assessing vitamin D status and it is used to define clinically meaningful states of vitamin D status, i.e. Deficient, Insufficient, Sufficient, and Toxic. However, the lack of standardized total 25(OH)D research data is the fundamental limitation in defining them. To correct that problem the Vitamin D Standardization Program (VDSP) has developed a reference measurement system, based on gold standard reference measurement procedures developed by the US National Institute of Standards and Technology (NIST) and Ghent University in Belgium, that can be used to standardize all current and future measurements of serum total 25(OH)D. In addition, it has developed methodology for standardizing stored serum samples. While it is impossible to standardize all of the old research, if stored serum samples from the small subset of key vitamin D research studies could be identified, it might be possible, using VDSP methodology, to standardize them. Such an effort might then permit the definition of clinically meaningful states of vitamin D status based on standardized total 25(OH)D values. Moving forward it is important, as well, for researchers to collect not only standardized values of serum total 25(OH)D but to consider the standardization or harmonization of the assays for new markers of vitamin D status as the field advances. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592 KEY WORDS: ■ 25-HYDROXYVITAMIN D ■ CAP ■ DEQAS ■ NIST ■ PT/EQA ■ VDSP ■ VITAMIN D
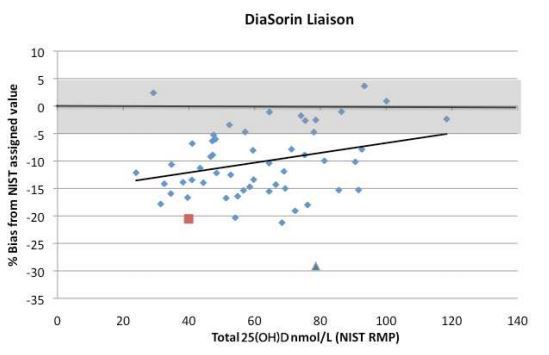
Introduction
The serum concentration of total 25-hydroxyvita- min D [25(OH)D] is considered to be the principal clinical marker for assessing vitamin D status1'2. As a result' much of vitamin D research has focused on determining the serum concentrations of total 25(OH)D which can be used to define clinically meaningful states of vitamin D status' i.e. Deficient' Insufficient' Sufficient' and Toxic.
An important event in vitamin D research was the development of the competitive protein binding assay (CPBA) for measuring total 25(OH)D in 19713'4. Since that time an ever increasing number of measurement procedures have been developed. Most of them are commercially available immunoassays. However' there was no gold standard assay method for measuring total 25(OH)D until 2011.
In 2010 and 2011 a series of events led to the development of reference measurement procedures (RMP) - gold standard assays - and a reference measurement system for standardizing the measurement of total 25(OH)D in both clinical and research laboratories. First, the US National Institute of Standards and Technology (NIST) and Ghent University developed RMPs and, more importantly, was the release by NIST of Standard Reference Materials (SRMs) that could be used to standardize routine clinical and research assays5-7 (Table 1). Second, anticipating those events, the Vitamin D Standardization Program (VDSP), founded in 2010, has developed a reference measurement system with the NIST- Ghent RMPs and the NIST SRMs as the cornerstone8 and embarked on an international effort to standardize the clinical and research laboratory measurement of total 25(OH)D around the world (Figure 1).* THESES *1. The lack of standardized total 25(OH)D measurement in Vitamin D research is the fundamental limitation thwarting the defining of clinically meaningful states of vitamin D status, i.e. Deficient, Insufficient, Sufficient, and Toxic.
The Vitamin D Standardization Program (VDSP) was founded in 2010 to correct this problem. VDSP has developed tools and methods for standardized measurement of serum total 25(OH)D in all clinical and research laboratories - both old research where stored serum samples exist and in all future research.
What do we do with all the old unstandardized 25(OH)D research data? Only a small subset of the published research tends to be key in guidelines development. Those key studies need to be identified and where possible standardized. Where that is not possible old studies may need to be repeated. In that way it may be possible to develop standardized consensus guidelines within a few years.
Finally, in all current and future vitamin D research the measurement of total 25(OH)D should be standardized using VDSP tools and methods.
The Problem
Between the years 1971 and 2015 approximately 60??? vitamin D research papers have been published. The rate is now about 5,000 per year. Unfortunately over those years, without standardization, there has been an enormous amount of variability both between and within the different assays used to measure total 25(OH)D9. This lack of standardized research data has made it difficult to pool the total 25(OH)D values from different key research studies in order to develop evidence-based clinical and public health guidelines for vitamin D and it may have helped to lead to differences between and among different sets of guidelines1'2. Stated unambiguously, that lack of standardized total 25(OH) D research data is the fundamental limitation in defining clinically meaningful consensus states of vitamin D status10.
The Ever-present Past
What do we do with all of the unstandardized total 25(OH)D research data? Do we continue to conduct meta-analyses and to develop clinical and public health guidelines using unstandardized and potentially biased data or do we just discard all of the old data and start anew? The practical solution to that problem is to identify and standardize the total 25(OH)D data from those key studies where stored frozen samples are available for re-analysis. That is, it may be possible to identify a small subset of all the prior research studies that are critical to guidelines development. Once identified it may be possible then to calibrate the 25(OH)D values from them to the NIST and Ghent University reference measurement procedures using VDSP methods thereby permitting future guidelines to be based on standardized results11'12. Where that is not possible it is recommended that medical and nutrition societies consider drawing up lists of research needing to be repeated.
For example, as part of the recently published Institute of Medicine Dietary Reference Intakes (DRI) for Calcium and Vitamin D, the DRI Committee concluded that a serum total 25(OH)D concentration > 50 nmol/L met the vitamin D requirements of 97.5% of the population needed to maintain bone health1. Subsequently, a small set of ten clinical trials of vitamin D supplementation on achieved 25(OH)D under minimal sun exposure were used to estimate the vitamin D intake such that 97.5% of all Americans would have a total 25(OH)D concentration > 50 nmol/L. Just the data from ten studies played an enormously prominent role in the development of the DRI Committee’s guidelines. What if the total 25(OH)D data from those ten studies could be standardized and those analyses repeated: would the recommendations be any different? Without standardizing those data it is impossible to know the answer to that question. However, that would only be the start. Standardized 25(OH)D data is essential to determine if there is a similarly small subset of total 25(OH)D data from key studies that could be used to characterize the relationship between total 25(OH)D concentration on the risk of rickets? What about osteomalacia, bone health indices, fracture risk, falls and muscle strength? If clinical and nutrition committees would define small subset of key studies in those different areas which need to be standardized it just might be possible in a few years to revisit the definition of the states of vitamin D status using standardized values of total 25(OH)D.* Breaking with the Past *The VDSP was designed to break with the past by providing tools and a methodology for standardizing the measurement of serum total 25(OH)D in both the clinical and research laboratories9,10. The tools include:
Reference measurement procedures from NIST and Ghent University
NIST Standard Reference Materials (Table 1)
Performance Standards: CV < 10% and Mean Bias < 5%
CDC Standardization Certification Program
Accuracy-based Performance Testing/External Quality Assessment (PT/EQA) through College of American Pathologists (CAP) Accuracy-Based Vitamin D (ABVD) Program and the Vitamin D External Quality Assessment Scheme (DEQAS)
Methodology for calibrating stored serum samples to NIST and Ghent RMPs
Those tools were designed for use to standardize the total 25(OH)D measurements made with any assay or measurement system. Accordingly, those tools should be used by researchers to standardize all current and future research measurements of total 25(OH)D.
With those tools the steps to standardization are to (Figure 1):
Calibrate commercial assays to NIST SRMs and/ or NIST and Ghent University RMPs.
Calibrate individual clinical and research assays to reference materials and RMPs.
Verify end-user performance through the CDC Standardization Certification Program and/ or CAP and DEQAS PT/EQA.
Standardization is especially difficult for the researcher as their assays are used intermittently. Therefore we suggest that researchers use the VDSP tools and repeat the steps to standardization prior to each period when the assay is to be used. To help in this process we recommend that researchers consider purchasing NIST SRMs and one or more sets of individual donor serum samples to assist in calibrating their assays. Individual patient samples with RMP assigned target values are the backbone of the CDC Vitamin D Standardization Certification Program13 and are available from CDC14. Limited numbers of DEQAS samples with target values assigned by NIST using their RMP are also available from DEQAS (www.deqas.org ).
For laboratories using a commercial measurement system, researchers should work with their representative to make sure that their assay is correctly calibrated to NIST and Ghent University. Mixing in blind samples of NIST SRMs or samples from DEQAS along with study samples can be used to assure calibration throughout the entire measurement process.
For those researchers who contract with other vitamin D researchers or with commercial laboratories to measure serum total 25(OH)D in their study samples, we recommend that you consider using only laboratories that have been CDC certified. The CDC website can be consulted for the current list of certified measurement procedures and laboratories14.* Will the Past be the Future? *Finally, vitamin D research is continuing to expand to include numerous other vitamin D metabolites. Currently, there is an enormous interest in 3-epi-25(OH)D, 24R,25(OH)2D3, vitamin D binding protein, bioavailable 25(OH)D, free 25(OH)D and cholecalciferol. Research in those areas may lead to those becoming important clinical markers. In addition, this new research opens the possibility that the very definition of vitamin D status may change in the future. As vitamin D research advances, the field needs to avoid the problems of lack of assay standardization that continue to plague research related to total 25(OH)D.
In anticipation of those new areas of research, the NIH Office of Dietary Supplements and NIST have collaborated to develop a laboratory methods research program. That program has led NIST chemists to develop a new assay for 24R,25(OH)2D3; it is hoped that this assay will be designated as an RMP. In the meantime, NIST is preparing certified values for 24R,25(OH)2D3 in SRM 972a and 2973 (Table 1). There are also plans to develop an ethanol-based SRM for 24R,25(OH)2D3 that can be used as a calibrator.
For metabolites where a reference measurement procedure does not exist, there may be a need to consider developing harmonization efforts to adjust all of the currently existing assays to a common value even though it is not known if that value is accurate15. Harmonized results can be adjusted over time as assay development takes places even to including an eventual reference measurement procedure. What is necessary is for the field to set priorities for harmonizing vitamin D metabolites and to work to secure the funding to make the realization of those priorities possible.
In summary
The lack of standardized 25(OH)D research data is the fundamental limitation in establishing clinical and public health vitamin D guidelines. With the advent of the VDSP, vitamin D researchers have been given the tools for standardizing the laboratory measurement of total 25(OH)D now and in the future. Moreover, tools have been developed that can be used to calibrate stored serum samples from old studies to the NIST and Ghent RMPs. What is needed is an effort to define those studies which are key to defining clinically meaningful states of vitamin D status, i.e. Deficient, Insufficient, Sufficient, and Toxic.
As vitamin D research identifies promising new ways of evaluating vitamin D status, work to develop new reference measurement procedures, reference materials, and standardization or harmonization strategies needs to proceed simultaneously with that research in order to avoid the problems of assay variability in the future. ■[email protected]
Assays for vitamin D metabolites; performance in the real world
Graham Carter, Julia Jones, Emma Walker
Clinical Biochemistry Department, Imperial College Healthcare NHS Trust, Charing Cross Hospital, London
DEQAS is an international external quality assessment scheme for 25-hydroxyvitamin D [25(OH)D] and 1,25-dihydroxyvitamin D [1,25(OH)2D]. The 25(OH)D scheme has approximately 1100 participants in 53 countries using 26 methods or variants of methods (April 2015). In April 2013, DEQAS became an accuracy - based scheme for 25(OH)D, with results being assigned to all samples by the Reference Measurement Procedure of the US National Institute of Standards and Technology (NIST). DEQAS participants are now able to compare the accuracy (bias) of their results with those of an internationally recognized reference method. Results given by many methods can be compromised by pre-analytical factors, by differences in the sample matrix and the presence in serum of other metabolites of vitamin D. Performance in routine clinical laboratories may not always reflect the claims made by kit manufacturers whose data is generally produced under the ideal conditions of their own laboratories. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592 KEY WORDS: ■ 25(OH)D ■ 24,25(OH)2D ■ DEQAS ■ REFERENCE MEASUREMENT PROCEDURES
Introduction
Vitamin D is the collective name for a group of substances having anti-rachitic activity. In humans the most abundant of the vitamins D is the naturally occurring vitamin D3 (cholecalciferol) made from the precursor 7-dehydrocholesterol by the action of sunlight on the skin. A second form, vitamin D2 (ergocalciferol) found in invertebrates and some foodstuffs is sometimes used, particularly in the US, to supplement vitamin D deficient subjects. Both forms of the vitamin are thought to be biologically inactive and undergo identical hydroxylations in the liver and kidneys to produce 25(OH)D and l,25(OH)2D respectively. The active form of the vitamin is l,25(OH)2D and, whilst the kidney is the major source of the hormone, it is also produced in many other tissues where it has autocrine and paracrine functions.* THESES *1. The containers in which blood is collected can influence 25(OH)D results.
Assay standardization and sample matrix can influence the accuracy and precision of 25(OH)D assays.
Cross reactivity of 24,25-dihydroxyvitamin D could falsely elevate 25(OH)D results in some assays.
Although 25(OH)D is not itself considered to be biologically active, its formation from vitamin D is unregulated and its concentration in serum is an accurate reflection of vitamin D intake1. Measurement of total 25(OH)D [25(OH)D3 plus 25(OH)D2] is universally used as an index of vitamin D nutrition and it is important that assays are co-specific for both metabolites when used for assessing subjects receiving a vitamin D2 supplement2.
DEQAS was established in 1989 after a national survey in the UK3 confirmed the wide inter-laboratory variation of 25(OH)D results previously observed in an international study4. With the support of the NIH Office of Dietary Supplements, the 25(OH)D scheme is now accuracy based; values are assigned to all DEQAS samples by the NIST Reference Measurement Procedure (RMP)5. A similar method is used by NIST to measure the metabolite 3-epi-25-hydroxyvi- tamin D3 [3-epi-25(OH)DJ. With about 1100 participants in 53 countries, DEQAS is ideally placed to assess the performance of different 25(OH)D methods in a wide range of routine clinical laboratories. From time to time, DEQAS conducts investigations into aspects of methodology that might affect the reliability and interpretation of 25(OH)D results.
Scheme Design
In brief, liquid samples5 prepared from pools of unadulterated human serum are sent out quarterly at ambient temperature. Participants are asked to measure total 25(OH)D and to return their results within approximately 5 weeks. Results are trimmed by removing the highest and lowest 5% to calculate the All-Laboratory Trimmed Mean (ALTM)6; the same trimming procedure is applied to the results of individual methods having 10 or more users. Since April 2013 the performance of individual participants is judged by the deviation (bias) of results from the value assigned by the NIST RMP (the ‘target’ value). Only the first 4 samples are used to assess performance; the fifth sample is reserved for specific investigations that can sometimes involve altering the serum matrix. A preliminary report, available on the DEQAS website, can be viewed by those participants who have returned results and the final report is published within about 2 weeks of the results deadline. A comprehensive summary of the recent performance of 25(OH)D and 1,25(OH)2D methods is available on the DEQAS website (www.deqas.org
This review will concentrate on three specific topics that have been addressed by DEQAS:
a pre-analytical problem;
Accuracy and precision;
24,25-dihydroxyvitamin D [24,25(OH)2D].
A pre-Analytical Problem
Until recently the serum pools used by DEQAS were prepared from blood obtained from patients undergoing therapeutic venesection for polycytha- emia or haemochromatosis. In 2013 the Haematology Clinic moved from London’s Charing Cross Hospital (where DEQAS is based) to the Hammersmith Hospital, a distance of 2 to 3 miles. Transport delays meant the blood often remained over night in the collection bags before centrifugation and harvesting of the serum.
In July 2013, NIST reported that all DEQAS samples from blood donated in the Hammersmith clinic contained a substance that apparently co-eluted with 3-epi-25(OH)D37 and produced an M/S peak overlapping that of the 3-epimer. This had not been seen in serum from Charing Cross donations and the most likely explanation was that something, possibly a plasticizer, was leaching from the collection bags. Information from the manufacturers (Fenwal Europe sprl, Belgium)) revealed that their collection bags contained the commonly used plasticizer Di (2-ethylhexyl) phthalate (DEHP). The bags used in the Hammersmith clinic were from the same manufacturer but were sterilized by gamma irradiation whereas the Charing Cross bags were steam sterilized.
It was later confirmed that DEHP was present in the DEQAS samples. However, DEHP has no structural similarities with 25(OH)D and further investigations by NIST effectively eliminated this as the interfering peak. It is likely that DEHP is simply a surrogate for other substances leached from the bags, of which there are many. Nevertheless, there was concern that the bias of some assays might be explained by the presence of the leached materials in DEQAS samples. This was investigated by simultaneously collecting some of the donated blood into plain glass tubes and subjecting them to the same transport and storage conditions as the bags. Measurement of 25(OH)D in the paired samples was performed with 5 commonly used automated ligand binding assays and a local LC-MS/MS method.
A comparison of results from blood collected into bags and glass tubes showed that only one method (the Siemens Advia Centaur) gave 25(OH)D concentrations that were significantly different (Table 1). Meanwhile DEQAS started to purchase serum from a US company (Solomon Park, Kirkland, WA) which collects blood according to C37-A
Table 1. Mean 25(OH)D results on blood collected
FIG. 1 The mean % bias from the NIST assigned value vs total 25(OH)D concentration in a series of DEQAS samples analysed by 5 fully automated ligand binding assays (A to E) and LC-MS/MS (F). Shaded area represents suggested bias limits for routine assays19 guidelines designed to minimize the presence of leached substances8. This has eliminated the interferent and also brings DEQAS into line with other accuracy-based schemes that use blood collected according to the same guidelines.Accuracy and Precision Whilst DEQAS results have shown improved agreement among participating laboratories over the last few years, the variability of results given by commercial methods can still be considerable9'10,11. Different approaches to the standardization of assays is clearly a potential factor in these discrepancies and the Vitamin D Standardization Program (VDSP)12 has been instrumental in persuading some manufacturers to harmonize standardization and to make their results traceable to an RMP. Several manufacturers have re-calibrated their assays and have obtained certification by the CDC Standardization-Certification Program13. Nevertheless differences among assays persist and there can also be considerable variability of bias among samples analyzed by the same method. This is illustrated in Figure 1 which gives the mean bias in a series of DEQAS samples analyzed by 5 fully automated ligand binding assays and LC-MS/MS. Two of the immunoassays (the Liaison and iSYS) show an overall negative and positive bias respectively and the LC-MS/MS mean is slightly positively biased against the NIST RMP, probably due to the inability of many LC-MS/MS methods to resolve 25(OH)D3 from 3-epi-25(OH)D3 which has the same mass14.
One sample had an endogenous triglyceride concentration of 4.0 mmol/L, about twice the upper limit of the local reference range. This apparently lowered the results of the immunoassays despite the level being below the interference threshold that most manufacturers state in their package inserts.
The results in Figure 1 also confirm the findings of previous DEQAS investigations, that some methods are not co-specific for 25(OH)D3 and 25(OH)D215. Whilst Abbott acknowledges low cross-activity (82%) of 25(OH)D2 in their Architect assay16), IDS and DiaSorin claim 100% cross-reactivity for the iSYS and Liaison assays respectively17'18.
Bias of results may be concentration-dependent and four of the ligand binding assays featured in Figure 1 have a positive association between bias and 25(OH)D concentration. Significantly, samples with higher concentrations of 25(OH)D are also likely to contain high levels of 24,25(OH)2D19, a metabolite known to cross react in all 25(OH)D immunoassays.
As with the leached materials from bags, the Siemens method is atypical. This method over-recovers 25(OH)D2 and shows a marked decline in bias with increasing 25(OH)D concentration. The reason for this is unclear but may be related to the specificity and affinity of the monoclonal antibody used in the Siemens assay.
24,25-dihydroxyvitamin D
In vitamin D replete subjects, 25(OH)D is preferentially hydroxylated to 24,25(OH)2D which can be regarded as a physiological mechanism to prevent hypercalcaemia . A genetic mutation in CY- P24A1 (24-hydroxylase) is now known to be the metabolic defect in idiopathic infantile hypercalcaemia21,22 and It has been suggested that the ratio 25(OH)D3: 24,25(OH)2D3 is a useful screening tool for CYP24A1 miutations in patients with hypercalcaemia19,22. For these reasons there has been a revival of interest in measuring 24,25(OH)2D, although currently this is probably mainly confined to research institutions.
Of more interest to most clinical laboratories is the potential interference of 24,25(OH)2D in assays for 25(OH)D. Because of the positive correlation between 24,25(OH)2D and 25(OH)D concentrations in human serum19, the concentration related bias seen in some ligand binding assays for 25(OH)D has been attributed to the cross-reactivity of 24,25(OH)2D23. However, an attempt at estimating cross reactivity by spiking a sample with 24,25(OH)2D was unsuccessful, producing unrealistically high results ranging from approximately 99% to 548% in the fully automated assays (Table 2). This did not reflect the observed concentration dependent bias in unspiked samples (Figure l and Table 3) and was probably due to the anomalous behaviour of exogenously added metabolite, as was observed with 25(OH)D24. Because of the current interest in 24,25(OH)2D, DEQAS is considering extending the scheme to include performance assessment of 24,25(OH)2D methods. To assess the degree of interest, participants were asked to measure 24,25(OH)2D as well as 25(OH)D on samples distributed in April 2015. Results were received from 7 laboratories and showed considerable variability (Table 4). Further data will be collected in forthcoming distributions.Discussion At first sight, the finding of an interferent leached from plastic blood collection bags is of little consequence to a routine clinical laboratory that would generally receive blood samples in hard plastic tubes. However, even hard plastic tubes are not immune from problems and the leaching of so-called slipping agents used in their manufacture has been implicated in causing ion suppression in LC-MS/MS assays25. In a wider sense, it is clearly important that samples distributed by proficiency testing schemes should closely mimic patient samples ie. should be commutable26'27. Blood from transfusion donor sessions is highly likely to contain materials leached from the collection bags and schemes using these donations should ensure that their samples are commutable for all the analytes being monitored. DEQAS samples were found to be commutable on the immunoaassay platforms studied in a recent survey undertaken by NIST and NIH on behalf of the VDSP28. DEQAS will participate in an expanded survey due to be conducted in March 201629.
The addition of exogenous 25(OH)D to enhance serum levels or the ‘processing’ of serum by some quality assessment schemes compromises the results given by many methods, so that performance can only bejudged within a cohort of participants using an identical method27. This approach is of limited value as it gives no indication of the absolute accuracy of the method or individual results, an important feature of accuracy-based schemes such as DEQAS. Published guidelines for the interpretation of 25(OH)D results such as those of the Institute of Medicine30 are not method specific and assume a degree of harmonization of results. The VDSP has had some success in promoting the common standardization of 25(OH)D methods among manufacturers but unfortunately this cannot address the observed variability of bias within the same method (Figure 1). This variability is probably due to so-called matrix effects to which non-extraction methods are particularly prone, a specific example being the falsely low 25(OH)D results in a sample containing a modest increase in triglyceride (Figure 1). Differences in vitamin D binding protein (DBP) have also been implicated in sample-to-sample variability of bias31. In demonstrating the variability of bias, the difference plots presented in Figure 1 are more effective than the regression plots generally used by manufacturers.
Manufacturers usually give some information about potential interference and cross reactivity of other molecules but this can sometimes be vague and lacking in experimental detail. Given the difficulties encountered by DEQAS and others in spiking serum with exogenous vitamin D metabolites24,32 manufacturers must be encouraged to be more transparent about how cross reactivity data is obtained and how their standards and controls prepared. The preparation of standards and kit controls in a matrix other than unadulterated human serum (such as horse serum) also requires justification in view of the apparent sensitivity of some methods to matrix differences. ■TAKE HOME MESSAGES 1. Pre-analytical factors such as the bags and tubes in which blood is collected can affect assay performance. Proficiency Testing schemes should ensure that their samples are commutable.
Participation in an accuracy- based external quality assessment scheme is a vital means of assessing and improving method performance and the accuracy of individual results.
The presence of dihydroxylated vitamin D metabolites [eg.24,25(OH)2D] may falsely elevate 25(OH)D results, particularly at high levels.
- Comparison of two immunoassays for vitamin D measurement is age a confounder?
Grażyna Odrowąż-Sypniewska, Joanna Siódmiak, Aneta Mańkowska-Cyl
Department of Laboratory Medicine, Nicolaus Copernicus University in Torun, Collegium Medicum in Bydgoszcz, Poland
The presence of different vitamin D metabolites in the circulation may contribute to the overestimation of 25(OH)D level, generally accepted to reflect vitamin D status, measured by some immunoassays compared to chromatography-based methods. There is an increasing interest in measuring the C3-epimer of 25(OH)D, which has shown to contribute significantly to the 25(OH)D concentration, particularly in infant populations, and in measuring the 24(R),25(OH)2D, a major catabolite of 25(OH)D metabolism. We aimed to present: a short description of analytical technologies quantifying 25(OH) vitamin D and some of its metabolites, some recent data on the contribution of vitamin D metabolites (3-epimers and 24,25(OH)2D) into total 25(OH)D results and a comparison of two different commercial automated immunoassays for 25(OH)D measurements in pediatric, adolescents and adult serum samples. Chromatography-based techniques that allow proper separation of 3-epimers and 24,25(OH)2D should be considered as the "gold standard"for 25(OH)D measurement. The cross-reactivity with 24,25(OH)2D in immunoassays may possibly contribute to some overestimation of 25(OH)D assay in adults and to the lesser extent in children, and both clinicians and laboratorians should be aware of this. Some immunoassays have no cross-reactivity with the 3-epimer and report only total 25(OH)D. Thus in samples that may have substantial amounts of 3-epi-25(OH)D LC-MS/MS or immunoassays showing no cross-reactivity with epimers should be recommended for assessment of vitamin D status to avoid overestimation of 25(OH)D and misclassification. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592
KEY WORDS: ■ 25(OH)D ■ VITAMIN D METABOLITES ■ LC-MS/MS ASSAYS ■ IMMUNOCHEMISTRY ASSAYS
Introduction
Synthesis of vitamin D in the human skin and subsequent liver and kidney metabolism generates a wide range of metabolites in very different concentrations. There are over fifty vitamin D metabolites of which 25(OH)D and l,25(OH)2D are well known to provide clinical information. The presence of different metabolites in the circulation may contribute to the overestimation of 25(OH)D level, generally accepted to reflect vitamin D status, by some immunoassays compared to chromatography-based methods. There is an increasing interest in measuring the C3-epimer of 25(OH)D, which has shown to contribute significantly to the 25(OH)D concentration, particularly in infant populations, and in measuring the 24(R),25(OH)2D, a major catabolite of 25(OH)D metabolism. The epimerization process seems to be a common mechanism for all major vitamin D metabolites. Epimers have identical structure but differ in stereochemical configuration.
Epimerization of 25(OH)D leads to overestimation of 25(OH)D concentration, independent of age, if the assay does not allow a proper separation of this stereoisomer. Similarly, the adjustment for concentration of 24,25(OH)2D seems to be an important issue, not only due to significant contribution of this compound to the serum total 25(OH)D.
This leads to the necessity of using selective and sensitive methods to quantitatively measure the concentrations of vitamin D metabolites in the blood. Ideally, vitamin D assessment would be performed using a universal and standardized analytical method available to clinical laboratories that provides reliable and accurate quantitative results for all relevant vitamin D metabolites with sufficiently high throughput1. There exists a wide diversity of assays for vitamin D from immunoassays to different chromatography assays combined with mass spectrometry. The accuracy of many commercially available immunoassays has been questioned. On the other hand, liquid chromatography combined with tandem mass spectrometry (LC-MS/MS) has been shown to facilitate not only accurate separation and quantification of the major circulating metabolite 25(OH)D3 and 25(OH)D2 but also other vitamin D compounds. Currently LC-MS/MS assays are the most promising techniques for the analysis of vitamin D metabolites. However, even these techniques are not free of influences of the biological matrix, contributions of epimers and isobars (such as exogenous la(OH)D3 and 7-a-hydroxy-4-cholesten-3-one, an endogenous bile acid precursor), derivatization reactions etc.
Theses: we aimed to present : a short description of analytical technologies quantifying 25(OH) vitamin D and some of its metabolites, some recent data on the contribution of vitamin D metabolites (3-epimers and 24,25(OH)2D) into total 25(OH)D results and a comparison of two different commercial automated immunoassays for 25(OH)D measurements in pediatric, adolescents and adult serum samples.
LC-MS/MS technologies for measurement of different metabolites of vitamin D in the human serum
Epimerization of vitamin D appears to be non-re- versible. Since C3-epimer of calcitriol was shown to have reduced calcemic effects measurement of 3-epi- 25(OH)D in addition to 25(OH)D seems to be of clinical importance.
The use of ultra-high-pressure liquid chromatography coupled to high-resolution mass spectrometry (LC/HRMS) showed that results for 25(OH)D3 can be affected by the inclusion of 3-epi-25(OH)D3 and it is important to separate this isomer from 25(OH)D32. Other technique, a liquid chromatography-triple quadrupole mass spectrometry -based method suitable for the quantification of 25(OH)D2 and 25(OH)D3 in human serum and plasma samples was shown not suitable for pediatric determinations due to the potential interference of 3-epi25(OH)D33. ESI-LC-MS/MS technique with the use of pentafluorophenyl (PFP) analytical column to resolve 25(OH)D3 from 25(OH)D2 and 3-epi-25(OH)D3 was shown to be accurate and allows the simultaneous measurement of 25(OH)D3, 3-epi-25(OH)D3, and 25(OH)D2 in human serum4. The authors noticed however, that due to increased ionisation efficiency, the contribution of the 3-epi- 25(OH)D3 metabolite to the total 25(OH)D3 concentration is significantly overestimated in MS methods that do not resolve 3-epi-25(OH)D3 from 25(OH)D3 and may compromise its use in infant samples known to have significant amounts of this isomer. Few current LC-MS/MS assays allow the accurate detection of C3 epimers5.Contribution of C3-epimers into the total 25(OH)D results The physiological importance of the C3 epimers of vitamin D is not well known, as are the demographic, behavioral, and physiologic factors that may be associated with their presence. So far, there have been limited studies determining the levels of these epimers in human populations.
Studies in infants have shown that 3-epi-25(OH)D3 can contribute 9-6l.l% of the serum total 25(OH)D36. High C3-epimer concentrations in infancy are probably due to postnatal formation of this isomer [7]. Bailey et al measured C3-epi- 25(OH)D3 by LC-MS/MS technique in pregnant women, fetuses and infants 3-28 weeks of age and found that C3-epi-25(OH)D3 accounted for up to 11% of maternal and 25% of infant total 25(OH)D3. C3-epimer was present in all pediatric subjects, but was significantly elevated below 1 year of age and dropped by 50% at 12months ofage8. 3-Epi-25(OH)D3 is present in the majority of human serum specimens across the age span, from neonates to over 80 yrs old, although its concentration is generally low, particularly in adults9. Interestingly, in sera with very similar 25(OH)D3 concentration, the ratio of epimer to 25(OH)D3 may vary. In another study it was reported that the percentage of the 3-epi metabolite relative to 25(OH)D3 in infants ranges from 15% to 41%, and in adults from 2.5% to 17%10.
The concentrations of C3-epimer reported in infants were in average 18.2 nmol/L (7.28 ng/mL) ranging from 0-230 nmol/L (0-92 ng/mL) and decreased after 1 year to the values typical in adults. C3-epimer concentrations in adults were relatively constant and remained from 0-22.5 nmol/L (9 ng/mL), in average 4.3 nmol/L (1.72 ng/mL)5. Accordingly, the proportion of C-3-epimer in relation to 25(OH)D3 was higher in infants 0-61% (mean 21.4%) than in adults 0-47% (mean 5.9%)5.
Recent data show that also a high proportion of adult subjects have detectable 3-epi-25(OH)D3. In general, adult individuals with lower total 25(OH)D3 tend to have a lower percent of 3-epi-25(OH)D3 relative to the total but this is not always the case. Baecher et al. simultaneously quantitated several metabolites: 25(OH)D2, 25(OH)D3, 24,25(OH)2D3 and C3-25(OH)D3 in 50 adult samples with clinically relevant concentrations of 25(OH)D3U. They have used HPLC-MS/MS technique with PFP column and found significant amounts of C-3-epimer in 78% of samples. The relative concentrations of C-3-epimer were 4-20% (average 7%) and correlated with 25(OH)D3 concentration. Lower proportion of C3-epimer was reported in Thai population, less than 10 % of the total 25(OH)D levels12. It was observed that age, gender, and living in a rural area were associated with the relative amount of 3-epi-25(OH)D3 to total 25(OH)D3 in this population.
The interesting findings from small epidemiological study in white adults (21-74 yrs), assessing the association between 3-epi-25(OH)D3 and the proportion of epimer to the total 25(OH)D3 in relation to vitamin D intake, sun exposure, waist circumference and some demographic and behavioral factors, were recently reported13. Higher alcohol intake and lower waist circumference were shown to be associated with higher concentration of 3-epi-25(OH)D3. Moreover, higher alcohol intake was associated with higher percentage of epimer in relation to 25(OH)D3. The authors noted that the associations of 3-epimer with summer season and vitamin D intake from supplements, observed in this study, could be driven partially by individuals with low 3-epi-25(OH)D concentration. Increase of age was not related to amount of 3-epimer or its percentage in relation to 25(OH)D3.
3-epi-25(OH)D was found in 90.2% of pregnant women and in 94.5% of pregnant women with diabetes mellitus type 1 (T1DM)14. Seasonal variation in maternal 3-epi-25(OH)D levels was evident in both groups. Maternal obesity had a significant negative impact on 3-epi-25(OH)D.
Recently, significant differences between health and disease with C3-epimers having the potential to relate to disease were reported15. The concentrations of 3-epi-25(OH)D3 were found to be significantly higher in patients with T1DM, rheumatoid arthritis and Alzheimer disease. Receiver operating characteristic curve analysis showed good sensitivity and specificity for using the 3-epi-25-hydroxyvitamin D concentration to predict disease status (AUC=
In general, C3-epi-25(OH)D3 is considered a minor metabolite in adults (Table 1). However, observed between-individual variation in the concentration of this epimer, coupled with variability of its detection by the different assay methods, confounds current efforts to accurately measure total 25(OH)D and impairs the ability to define vitamin D status16. Wiebe and Binkley reported on three different patients: 66 yrs old female with multiple sclerosis, 7 yrs old boy with multiple medical comorbidities and 55 yrs old female with combined hyperlipidemia and hypertension, all with increased concentrations of 3-epi-25(OH)D and substantially increased proportion of epimer in relation to total 25(OH)D. Vitamin D metabolites were measured in the same clinical laboratory with quality assurance programme over the past 5 years. Interestingly, the proportion of 3-epimer to total 25(OH)D ranged from 25% in the young patient to 94% in the oldest one. The authors explain between-individual differences in epimerases activity by possible genetic factors.
Although the ratio of 3-epimers to 25(OH)D differs across the population age and health status, the considerable prevalence of 3-epi-25(OH)D3 in infants and in adults, proves this metabolite should not be neglected in interpretation of vitamin D results. In addition, it would be interesting to elucidate the possible associations of low, moderate or high concentrations of 3-epimers with health risk, independent of 25(OH)D3 or 1,25(OH)2D3 concentrations in different age groups6.
Contribution of 24,25(OH)2D into the total 25(OH)D results
The first downstream metabolite of 25(OH)D is 24,25(OH)2D which has its own physiological role for bone healing after fracture17 and essential bioactive role in human bone development as recently reported18. Its concentration in the serum may account for 2% up to 20% of total 25(OH)D19. Earlier studies in children and adolescents have shown that serum concentration of 24,25(OH)2D relative to total 25(OH)D was up to 10% and equaled to 3,3+/-1.3 ng/mL20. Recently reported levels of 24(R),25(OH)2D, a metabolically active natural form of this metabolite, seem to be slightly higher in healthy adults than in children and adolescents (0.7-24 nmol/L or 0.28-9.6 ng/mL) (Table 2)21. Of note, concentrations of 24,25(OH)2D were found to be significantly lower in some disease states, such as multiple sclerosis, compared to healthy individuals21.
Calculated ratio of 24,25(OH)2D to 25(OH)D, so called vitamin D metabolic ratio, is considered a novel index of vitamin D deficiency and possibly inactivation and a novel predictor of 25(OH)D response to vitamin D supplementation21. Currently, there are no automated immunoassays for determination of 24,25(OH)2D thus measurement of vitamin D metabolic ratio is available only in laboratories with LC-MS capabilities.Comparison of two different commercial automated immunoassays for 25(OH)D We compared the results of total 25(OH)D measured in serum samples of subjects aged of 2-70 years, with two different commercial immunoassays: Roche cobas e411 and ids iSYS. The first, a 1-step competitive binding against vitamin D binding protein electrochemiluminescence assay is standardized with NIST SRM 2972. The second, a 1-step competitive binding against 25(OH)D chemiluminescence assay is standardized with UV verified by LC-MS/MS. Both immunoassays have very similar LOD (3.0 and 3.6 ng/mL respectively) but different linearity: 3.0-70 ng/mL and 6.0-126 ng/mL, respectively. The ids iSYS assay is known to have no cross-reactivity with 3-epimers but presents 100% cross-reactivity with 24,25(OH)2D. The cross-reactivity of the Roche assay with 3-epimers is 91% and with 24,25(OH)2D is 149% according to the kit insert.
Interestingly, recently published data by van den Ouweland et al on evaluation of 3-epi 25(OH)D3 cross-reactivity in the Roche vitamin D total protein binding assay showed that the cross-reactivity over 50% was found with exogenous 3-epimer 25(OH)D3 whereas this with natural endogenous metabolite was minimal22. The authors conclude that more research is needed to help explain the discrepancies in 3-epimer recognition by the method between endogenous and exogenous presence of the 3-epi 25(OH)D322.
Our preliminary results have shown that there are differences in 25(OH)D total concentrations measured by both immunoassays in the serum samples across the different age-groups.How to optimally measure 25(OH)D in the laboratory Over recent years a dramatic increase has been observed in 25(OH)D requests. Automated immunoassays helped many laboratories to solve this problem. In these methods with high throughput the traditional solvent extraction of samples was abandoned. Comparing with LC-MS/MS, immunoassays for 25(OH)D measurement are more affordable due to economic and organizational issues and require small sample volume, particularly convenient for pediatric testing. However, poor antibody specificity with cross-reactivity to other vitamin D metabolites, incomplete extraction of the 25(OH)D from the vitamin D-binding protein (DBP), and confounding matrix substances such as lipids (increased triglycerides) could be potential reasons for the unsatisfying performance of some immunoassays and also the significant differences in the 25(OH)D results between various assays23. In spite of these, immunoassays should be regarded as an alternative for routine 25(OH)D assessment, provided that results are accurate and correlated with a reference method24. Recent multicenter comparison of seven 25(OH)D automated immunoassays has shown the very good correlation with the reference HPLC method23. However, the significant bias among different methods shows that standardization and harmonization of 25(OH)D measurements are urgently needed.
Some currently available immunoassays allow detection of C3 epimers along with 25(OH)D (Roche 25(OH)D total) whereas some do not recognize epimers (ids i-Sys, idsEIA, Abbott Architect). In several
1. Pleiotropic action of vitamin D in light of recent meta-analyzesIdris Guessous1,2,3
Unit of Population Epidemiology, Department of Community Medicine and Primary Care and Emergency Medicine, Geneva University Hospitals, Geneva
Institute of Social and Preventive Medicine (IUMSP), Lausanne University Hospital, Lausanne
Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta
The relationship of vitamin D with extraskeletal complications, such as cardiovascular disease, cancer, and autoimmune disease, is of major interest considering its roles in key biological processes and the worldwide high prevalence of vitamin D deficiency. Several arguments suggest a major role of vitamin D in a very broad type of extraskeletal complications, but results from recent meta-analyses of randomized controlled trials indicate a lack of association of vitamin D with major extraskeletal complications. Different issues including causality, confounding, reverse causation, and misclassification should be considered when interpreting these opposite conclusions. Randomized controlled trials assessing the efficacy of vitamin D supplementation in reducing extraskeletal complications are ongoing. Trials are still recruiting participants, and the first results will not be available before the year 2017. Unfortunately, because of potential major limitations, results from these trials might not be able to definitively determine the causal role of vitamin D on extraskeletal complications. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592 KEY WORDS: ■ VITAMIN D ■ CANCER ■ CARDIOVASCULAR DISEASE ■ EVIDENCE ■ CAUSALITY
In humans, most circulating vitamin D is synthesized from cholesterol following exposure to ultraviolet B (UVB) in sunlight, whereas a smaller amount is derived from diet and dietary supplements. Diet contributes only between 10% and 20% to 25(OH)D levels but becomes more important when sunshine exposure is low1. The actions of vitamin D are largely mediated by genomic functions. Vitamin D interacts with a nuclear receptor that regulates the expression of over 900 genes throughout the genome2.
Currently, a debate over the role of vitamin D on extraskeletal complications is being conducted3.
The rational of a major role of vitamin D on extra- skeletal complications is based on several observations including:
the worldwide high prevalence of vitamin D deficiency is often presented as being clearly linked with the high burden of extraskeletal complications,
vitamin D is often presented as the link explaining most of the observed correlations between latitude and season with extraskeletal complications,
the wide distribution of vitamin D receptor in humans,
the influence of vitamin D on more than 3% of the human genome,
the extrarenal presence of 1-alpha-hydroxylase.
In addition, molecular and animal studies have established associations of vitamin D with several extraskeletal complications including cardiovascular disease such as high blood pressure, coronary heart disease, and stroke, type II diabetes, cancer, and chronic kidney disease.
Despite this evidence, there is a belief that vitamin D is not causally associated with extraskeletal complications. This belief is mainly based on the absence of robust evidence of this association from randomized controlled trials (RCTs), on the potentially unfavorable effects of vitamin D supplementation, and on the precedents of other vitamin and antioxidant trials. To date, most associations of vitamin D with extraskeletal complications reported by nonexperimental studies have not been replicated in RCTs. To evaluate the presence of biases in the associations of vitamin D with diverse extraskeletal outcomes, a review of evidence obtained from systematic reviews and observational meta-analyses and RCTs (i.e., an umbrella review) has been performed4. More than 260 systematic reviews or meta-analyses that have included over 130 outcomes have been examined. The authors reported a lack of highly convincing evidence of a clear link of vitamin D with any outcome. The most recent (2011) meta-analysis has concluded that because of the potential confounding data inherent in observational studies and the limited data obtained from RCTs, evidence is currently insufficient to draw conclusions about the efficacy of vitamin D supplementation for cancer prevention5. A 2014 review of vitamin D status and cardiovascular disease by the UK Nutrition Society has concluded that data supporting a causal link between vitamin D status and CVD are mixed and ambiguous6. Similar conclusions were independently published in 2011 by the North American DRI committee7, by the Endocrine Task Force8, and more recently, by others9-13. In terms of endocrine health and disease, available evidence does not show that vitamin D supplementation consistently decreases the risk of type II diabetes, Addison’s disease, or autoimmune thyroid disease14.
While a 2014 meta-analysis of observational studies of vitamin D and mortality caused by extraskeletal complications found evidence that 25(OH)D level is inversely associated with risk of death due to extra- skeletal complications, no evidence of such a relationship has been found in RCTs15. Even Mendelian randomization (MR) studies have been conducted to infer causality for vitamin D and extraskeletal
complications, such as high blood pressure and type II diabetes. For example, Kunutsor et al. have used 4 variants (in the DHCR7, CYP2R1, GC, and CYP24A1 genes) as instrumental variables in a small sample, failing to show a causal role of 25(OH)D in the etiology of high blood pressure16. Using the same 4 variants but considering allelic scores and using a larger sample, Vimaleswaran et al. reported that each 10% increase in genetically instrumented 25(OH)D concentration was associated with an 8% decreased odds of hypertension17. However, using the same variants as mentioned above but not considering allelic scores, Ye et al. have also estimated the unconfounded causal associations of 25(OH)D concentration with the risks of type II diabetes and other glycemic traits using an MR approach18, reporting insignificant MR-derived estimates for type II diabetes and glycemic traits and suggesting that the association between 25(OH)D and type 2 diabetes is not causal.Key points There are several major issues to consider when interpreting the real impact of vitamin D deficiency on extraskeletal complications. These issues include causality, confounding, reverse causation, measurement error and misclassification. To overcome these issues, five RCTs are currently underway in 9 countries to determine the impacts of vitamin D supplementation on extraskeletal complications. More than 42,000 participants will be included with a potential of 208,116 person-years. However, several experts have already pointed out fatal limitations that might invalidate the (negative or null) results of these trials. Also, a 2014 trial sequential meta-analysis (i.e., analysis that modeled the changing precision in estimates of effects as trials are reported and the likely effects of future trial results on the existing body of data) has shown that the effects of vitamin D supplementation on extraskeletal complications are below the futility boundary of 15%9'19. Thus, future trials are unlikely to alter the conclusion of no causal association.
Observational studies are prone to reverse causation and confounding. Associations between vitamin D status and extraskeletal complications in observational studies could merely indicate that vitamin D is a “simple” indicator of health status and that compared with healthier subjects sicker subjects could have a lower vitamin D level or status. The diversity of biological systems with which vitamin D deficiency has been associated (cardiovascular, diabetes, depression, neurodegenerative diseases, cancer, etc.) could further suggest that this vitamin is a marker of health status rather than a predictor of health outcomes. However, both the wide distribution of VDRs in humans and the influence of vitamin D on more than 3% of the human genome could explain its broad effects on health.
Unfortunately, results from the ongoing randomized controlled trials might not be able to definitively determine the causal role of vitamin D on extraskeletal complications3. ■
1. Vitamin D Requirements during Pregnancy and LactationBruce W. Hollis, Carol L. Wagner
Medical University of South Carolina, Charleston
During the past several decades, vitamin D requirements during pregnancy and lactation were unvarying, with the recommendation for a daily vitamin D intake of 400 IU. During the past decade, however, mounting evidence suggests that maternal vitamin D requirements during these critical stages are much greater. There are important differences in vitamin D metabolism during pregnancy and lactation that impact maternal, fetal and infant health. A summary of relevant clinical trials that have been conducted to answer the question of what amount of vitamin D is necessary to optimize vitamin D metabolism during pregnancy and lactation suggests maternal intake during pregnancy is optimized at 4000 IU vitamin D/day and during lactation at 6400 IU vitamin D/day. Further research is essential to establish the mechanisms of action of vitamin D in immune function and optimal health. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592 KEY WORDS: ■ PREGNANCY ■ LACTATION ■ VITAMIN D
Introduction
Vitamin D’s actions during pregnancy and lactation reflect its role as a preprohormone, serving as the substrate for one of the most potent hormones in the body -l,25(OH)2D, whose nontraditional endocrine effects are just beginning to be understood. Until the 1990s, the criterion for appropriate vitamin D nutrition was simply the absence of overt rickets or osteomalacia1. An expert panel convened by the Institute of Medicine in 1997 recommended that infants and adults receive 400 and 200 IU/day vitamin D, respectively, in the prevention of rickets and osteoporosis2, reflecting the time-honored observation that one teaspoon of cod liver oil (which contains 400 IU vitamin D3) is effective in preventing rickets in children3,4. The daily vitamin D dose for adults of 200 IU in achieving vitamin D sufficiency without adequate sunlight exposure was later shown to be inconsequential in all but the most deficient adult individuals5,6, with even less known about the needs of the pregnant and lactating woman and that of the developing fetus and breastfed infant2,7.
With the newly found ability to measure vitamin D and its metabolites in the 1980’s, it became evident that certain groups of women, especially those of darker pigmentation or with limited sunlight exposure due to clothing worn for cultural reasons, were vitamin D deficient8-15. Trials involving doses up to 1000 IU/day were shown to do little to reverse that deficiency8-10,16-19. There was a resurgence of reports of vitamin D-associated rickets among exclusively breastfed infants, particularly those who had darker pigmentation20-22 and led some to question whether or not a prenatal vitamin containing between 200-400 IU vitamin D taken during pregnancy and lactation was adequate with today’s lifestyles23'24. This was underscored by a paper published by the Center for Disease Control (CDC) in 2002 on the prevalence of vitamin D deficiency among women in their child bearing years: Utilizing the Third National Health and Nutrition Examination Survey' 1988-1994 (NHANES-III) database' Nesby-O’Dell and her team measured total circulating 25(OH)D in 1546 African American women and 1426 white women aged 15-49 y who were not pregnant24. Hypovitaminosis D was defined as a serum 25(OH)D concentration <15 ng/mL (37.5 nmol/L). More than 40% of the African American women in this large cohort met the criterion for vitamin D deficiency having a 25(OH)D concentration of < 37.5 nmol/L compared to 4.2% of white women 24. In addition' among the 243 African Americans who consumed 200 IU/d' ~28% met the definition of hypovitaminosis D.
Emerging literature from the 1980’s showed that with severe vitamin D deficiency states' fetal growth impairment was noted8'13.
Earlier literature suggested that not only growth was impacted by vitamin D deficiency: in the early 1900’s' Mellanby and others25-27 in their study of vitamin D deficiency in children and in animal models found an increased risk of respiratory infections' but even Mellanby (and his colleagues) discounted the effect of vitamin D on infection risk28. It took another 60 years before the (re)discovery of vitamin D’s role in immune function set the stage for an expansion of scientific inquiry into vitamin D’s role in immune function in an unprecedented manner29-35. Elaboration of inflammatory and immune markers as a function of vitamin D status led some to consider higher target concentrations of vitamin D were necessary to maintain optimal health' but again' little was known and remains unknown about the role of vitamin D during pregnancy and lactation on immune function and what normal really was.
The evidence continued to mount that there were far more deficient or marginally sufficient pregnant women than there were vitamin D sufficient pregnant women36-41, but there was concern that this was not “true” deficiency and the increasing prevalence was occurring because of a different set point in defining vitamin D deficiency. Controversy arose surrounding what moiety of vitamin D defined deficiency; eventually the scientific community agreed that the concentration of total circulating 25(OH)D was the indicator of vitamin D sufficiency (due to its longer half-life of 2-3 weeks and its relative ease of measurement. The next question then became what should 25(OH)D concentrations really be42,43?Vitamin D Metabolism during Pregnancy Vitamin D is the precursor to 25(OH)D that is then metabolized further by the kidneys and the placenta to the active form 1,25(OH)2D. It has been known for some time that circulating 25(OH)D freely crosses from maternal circulation to fetal circulation via the placenta, which possesses vitamin D receptors and the enzyme CYP27B1, essential for the conversion of 25(OH)D to 1,25(OH)2D44. While the kidneys are the main source of 1,25(OH)2D throughout the lifespan, the placenta does contribute to the pool of vitamin D metabolites that surge through both maternal and fetal circulations.
In their recent review of vitamin D, Hollis and Wagner point out, however, that the parent compound vitamin D plays a significant role in providing substrate to cells for internalization45: Vitamin D is vastly more accessible than 25(OH)D for internalization throughout the body with the exception of cells in the kidney and parathyroid gland, for example, that utilize the megalin-cubilin system46, and which maintain the vitamin D endocrine system. Cells that process vitamin D through paracrine/autocrine actions are dependent on delivery of vitamin D substrate and how tightly bound it is to the carrier protein vitamin D binding protein45. For example, circulating 25(OH)D’s availability to cells is reduced because it is tightly bound to the vitamin D binding protein (VDBP). In contrast, vitamin D is far more bioavailable as it is less tightly bound to VDBP, allowing entrance of vitamin D into the cell more easily than 25(OH)D. Once in the cell, vitamin D is then converted to 25(OH)D and then to its active form 1,25(OH)2D. There is no evidence to suggest that this is altered during pregnancy, although the concentration of VDBP during pregnancy is increased47. With respect to the conversion of vitamin D to 25(OH)D, this metabolic conversion appears to be similar in pregnant and nonpregnant states and follows first- and zero-order enzyme kinetics (Figure 1)48.
In any discussion about vitamin D deficiency, parathyroid hormone (PTH) is mentioned because PTH upregulates 1-a-hydroxylase, the enzyme responsible for 1-a-hydroxylation of 25(OH)D, converting 25(OH)D to 1,25(OH)2D. In individuals who have vitamin D deficiency, the body increases production of PTH to maintain 1,25(OH)2D and calcium homeostasis. If vitamin D deficiency is sustained, secondary hyperparathyroidism will result. Yet, during pregnancy, this association is diminished due to the uncoupling of vitamin D metabolism from calcium48. Pregnant women attain “su- praphysiologic” concentrations of 1,25(OH)2D in the first weeks of gestation49, sometimes exceeding 700 pmol/L in our NICHD study36, and yet never exhibit hypercalciuria or hypercalcemia. It is not surprising, then that during pregnancy PTH as a marker of vitamin D status is a less reliable predictor than in nonpregnant adults50 and typically will decrease as 25(OH)D increases at the lower end of values48'50'51.
What was most interesting from our recent NICHD vitamin D pregnancy trial was the discovery that to optimize 1,25(OH)2D production (which as was just discussed, soars early-on in pregnancy), total circulating 25(OH)D should be at least 100 nmol/L48. This relationship exhibits first and zero-order enzyme kinetics. It is also of great interest that production of circulating 1,25(OH)2D in the fetus is linked directly to circulating 25(OH)D52. This increase in circulating 1,25(OH)2D concentration has been attributed to an increase in the serum vitamin D-binding protein (DBP) that would regulate the amount of “free” 1,25(OH)2D available in the circulation53. While this rise in DBP during pregnancy has been shown to be 46-103 %, depending on the assay employed54, it cannot account for the 2-3 fold increase in circulating 1,25(OH)2D48. In an earlier study by Bikle et al.47, free 1,25(OH)2D levels were found to be increased during pregnancy despite the significant increase in DBP levels, and our recent data agree with this premise48. Why this association exists solely during pregnancy remains unclear and is the focus of active research endeavors.
As a corollary to the extraordinary change in vitamin D metabolism during pregnancy, it has been known for some time that unique during pregnancy, maternal and neonatal 25(OH)D and 1,25(OH)2D are strongly associated52. From early in gestation, serum 1,25(OH)2D concentrations rise much higher and are driven by substrate-25(OH)D-availability. It is important to again note that this substrate dependence of 1,25(OH)2D production is never observed in normal human physiology driven by classic calcium homeostasis nor is it seen in any other time in the lifecycle except pregnancy and in the newborn infant.Achieving Sufficiency during Pregnancy: Results of Clinical Trials through the Decades When considering what is the “norm” for vitamin D status, Luxwolda et al.55 studied native tribal Africans who have an average of 5-9 hours of sunlight exposure per day. This group achieved a mean circulating 25(OH)D level of 46 ng/mL (115 nmol/L). In another study by this group that included 139 East African pregnant women, the mean 25(OH)D was 55.4 ng/mL (138.5 ±31.8 nmol/ L) during pregnancy; and 54.4 ng/mL (135.9 ± 31.8 nmol/L) at delivery56. The cord blood 25(OH)D concentration was 31.6 ng/ mL (79.0 ± 26.4 nmol/L), well above the mean of cord blood values found in Western countries 48'57'58. On the third day postpartum, mothers-the vast majority who were breastfeeding, had a mean 25(OH)D of 91.5 ± 26.8 nmol/L that remained stable at 3 months postpartum. In our recent randomized clinical trial, pregnant women receiving 4,000 IU/day vitamin D3 attained an average circulating 25(OH)D level of 111 nmol/L48, similar to what is achieved through sunlight alone with a certain level of sun exposure. If one wants to recapitulate what occurs in individuals living in a sun-rich environment with hours of exposure, the goal should be to achieve a circulating 25(OH)D concentration of at least 100 nmol/L however it is achieved, be it solar exposure and/or diet/supplementation.
Following receipt of an Investigational New Drug (IND) number from the FDA (#66,346), Hollis and his team began to assess the vitamin D requirements of women during their first trimester of pregnancy. In their two published randomized controlled trials, Hollis et al and Wagner et al found that higher total circulating 25(OH)D was associated with improved vitamin D status throughout pregnancy48,59. In the first trial sponsored by NICHD, women were randomized to receive 400, 2000 or 4000 IU vitamin D3/day starting at 12 weeks of gestation48. Women were followed monthly to assess health status and vitamin D-re- lated metabolic parameters. It was found that 4000 IU/day vitamin D was superior to 2000- or 400 IU/ day, and 2000 IU/day was superior to 400 IU/day in achieving vitamin D sufficiency throughout pregnancy. Women taking 400 IU/day vitamin D had minimal change in their 25(OH)D concentrations; those in the 2000 IU group were often deficient through 20-24 weeks compared to the 4000 IU group. The number of neonates who were deficient at birth defined as a total circulating concentration of 25(OH)D <20 ng/mL was greater in the lower dose groups. There was no toxicity associated with the higher vitamin D dosing: women in the three treatment groups did not differ in terms of serum calcium, phosphorus, creatinine, and urinary calcium-to-creatinine ratios.
In another trial funded by the Thrasher Research Fund and conducted by Wagner et al.58, women who received their health care in two community health centers were randomized to receive either 2000 or 4000 IU vitamin D3/day starting at 16 weeks of gestation following a one-month run-in dose of 2000 IU/day. A total of 257 pregnant women 12-16 weeks’ gestation were enrolled and randomization to 2000 vs 4000 IU/day following a 1-month run-in dose of 2000 IU/day. As in the NICHD trial described above, participants were monitored for hypercalciuria, hypercalcemia, and 25(OH)D status. Maternal 25(OH)D (n = 161) increased from ~23 ng/mL (57.5 nmol/L) at baseline to 36 ng/mL (90 nmol/L) and 38 ng/ mL (95 nmol/L) in the 2000 and 4000 IU groups, respectively. While the change in maternal 25(OH)D from baseline did not differ between the groups, the increase in monthly 25(OH)D differed between the groups with the greater change in the 4000 IU group (p < 0.01). No supplementation-related adverse events occurred. Mean cord blood 25(OH)D was 22 ng/mL (55 nmol/L) in 2000 IU and 27 ng/mL (67.5 nmol/L) in 4000 IU groups (p = 0.024).
Both the NICHD and the Thrasher Research Fund pregnancy vitamin D supplementation trials utilized common questionnaires and vitamin D tablets from the same manufacturing lot, allowing the two datasets to be combined using a common data dictionary, increasing the sample size and power to detect differences between the groups59. It was again found that 4000 IU/day vitamin D was superior to either 400 or 2000 IU/day in achieving vitamin D sufficiency throughout pregnancy.
Other trials conducted throughout the world support the effectiveness of higher vitamin D dosing regimens in improving maternal vitamin D status. In a study conducted in the United Arab of Emirates by Dawodu et al60, Arab women were randomized at 12-16 weeks of gestation to 400, 2000, and 4000 IU/day vitamin D, through pregnancy. Of 192 enrolled, 162 (84%) continued to delivery. Mean serum 25(OH)D of 8.2 ng/mL (20.5 nmol/L) at enrollment was consistent with severe deficiency. Mean serum 25(OH)D concentrations at delivery and in cord blood were significantly higher in the 2000 and 4000 IU than the 400 IU/d group (p < 0.001) and was highest in the 4000 IU/d group. When using the threshold 25(OH)D concentrations of 32 ng/mL (80 nmol/L) and 20 ng/mL (50 nmol/L), the percent of mothers who achieved these thresholds was greatest in the 4000 IU/d group. Safety measurements were similar by group and no adverse event occurred that was related to vitamin D supplementation. The investigators concluded that vitamin D supplementation at doses of 2000 and 4000 IU/day appeared safe, and similar to the Hollis et al study, 4000 IU/d was most effective in optimizing serum 25(OH)D concentrations in mothers and their infants.
Roth et al reported the results of a clinical trial conducted in Dhaka where 160 women were randomized to receive 35,000 IU/week (=5000 IU/day) or placebo until delivery. Maternal mean 25(OH)D was significantly higher at delivery after vitamin D vs. placebo (134 vs. 39 nmol/L, P<0.001; N=133); and as expected, cord 25(OH)D was significantly higher following vitamin D versus placebo (103 vs. 39 nmol/L; P<0.001; N=132). In this study, there was no evidence of maternal hypercalcemia or vitamin D-related serious adverse events; and, major adverse birth and neonatal outcomes were non-significantly less common in the vitamin D-treated group.Health Effects of Vitamin D during Pregnancy As was mentioned earlier, what is unique during pregnancy is that total circulating concentrations of 1,25(OH)2D are more than double to triple by 10-12 weeks of gestation what they are in the nonpregnant state48. Despite this dramatic increase in the active hormone, serum calcium concentrations remain stable and within normal range. How could this be and more importantly, why does this occur? It is postulated that the sustained high concentration of 1,25(OH)2D during pregnancy serves an important role in stabilizing immune function in the mother to prevent rejection of the fetus61,62. Yet, this remains conjecture at this point because the discovery of vitamin D’s role in both innate and adaptive immune function is a relatively recent discovery33,63. There is, however, mounting evidence that supports this premise: women who are vitamin D deficient are more likely to have preeclampsia64-68, infection58,69,70, preterm labor and preterm birth58,59,71, all of which have been associated with states of vitamin D deficiency.
When randomized clinical trials or comparative effectiveness trials involving vitamin D supplementation during pregnancy have been analyzed for vitamin D’s putative effect on maternal and fetal health, certain trends have emerged. The first hint that vitamin D deficiency during pregnancy impacted fetal development came from studies conducted in the early 1980s. Brooke et al8,16, who studied British mothers of Asian descent, found a greater incidence of small-for-gestational-age infants born to mothers who received placebo compared with mothers who had received 1000 IU vitamin D2/day during the final trimester of pregnancy. Neonates in the placebo group also had a greater fontanelle area than did the supplemented group. It must be noted that the placebo group in this study showed profound hypovitaminosis D.
Follow-up studies by Brooke et al9 again were conducted in Asian mothers who were provided with either placebo or 1000 IU vitaminD2/day during the last trimester of pregnancy. The follow-up data provided evidence that, during the first year of life, the infants of the maternal placebo group gained less weight and had a lower rate of linear growth than did the infants of the maternal supplemented group. Cockburn et al72 undertook a large vitamin D supplementation study of 1000 pregnant subjects in the United Kingdom who were supplemented with 400 IU vitamin D2/d or received a placebo from week 12 of gestation onward. Based on pharmacokinetics of vitamin D, it is not surprising that serum concentrations of 25(OH)D in the supplemented group were only slightly higher than those in the placebo group. A defect in dental enamel formation was observed in a higher proportion of the children at 3 y of age in the maternal placebo group.
Maxwell et al84 conducted a clinical trial involving Asian women living in London who received 1000 IU/day of vitamin D during the last trimester of pregnancy. Supplemented mothers had greater weight gain and, at term, had significantly higher plasma concentrations of retinol-binding protein and thyroid-binding prealbumin, indicators of protein-calorie nutritional status. Almost twice as many infants of the unsupplemented group weighed < 2500 g at birth and had significantly lower retinol-binding protein concentrations than did infants of the supplemented mothers.
Brunvard et al 86 followed 30 pregnant Pakistani women who were free of chronic diseases and had uncomplicated pregnancies. Nearly all of the women had low (< 15 ng/mL) circulating 25(OH)D concentrations, and nearly 50% exhibited secondary hyperparathyroidism. The maternal circulating parathyroid hormone concentration was inversely related to the neonatal crown-heel length. These authors concluded that maternal vitamin D deficiency affected fetal growth through an effect on maternal calcium homeostasis.
Similar effects of vitamin D status on fetal growth were found in a more recent study by Hashemipour et al73 in their randomized controlled trial of 160 healthy pregnant women, of whom 81% were vitamin D deficient at baseline. This team of investigators based in Iran studied the effect of vitamin D administration on maternal and neonatal serum calcium and vitamin D concentrations. Women were randomized to receive a daily multivitamin containing 400 IU plus 200 mg elemental calcium (control group) vs. 50,000 IU oral vitamin D3 every 2 weeks for a total of 8 weeks starting at 26-28 weeks of gestation as well as the daily intervention given to the control group (average daily total of 3971 IU/day). At delivery, maternal 25(OH)D was significantly higher in the intervention group. Maternal weight gain during pregnancy was greater in the invention group and significantly correlated with serum 25(OH)D and inversely correlated with BMI at the time of enrollment. Growth parameters in the neonates of mothers in the intervention group were significantly greater than neonates in the control group, effects that persisted even after controlling for other maternal factors such as age, BMI, gravidity and gestational age at delivery. These findings are supported by earlier as well as more recent studies: Marya et al14 in 1988 and Kalra, et al74 in 2012 showed improved growth effects of vitamin D interventions as a function of timing during gestation as either a single large bolus of vitamin D given in the second trimester or two boluses during the second and third trimesters. In contrast, Mallet et al, who randomized women to receive 0, 200 or 1000 IU vitamin D/day showed no effect on neonatal weight. Based on the aforementioned studies, it would appear that the baseline starting 25(OH)D and the resulting 25(OH)D concentration that is achieved are the two predictors of fetal growth effect. There may be a threshold 25(OH)D concentration above which no further effect is seen in neonatal growth. In both the NICHD and Thrasher Research Fund trials, there were no differences in neonatal anthropometric measures, as a function of maternal vitamin D treatment, but those studies where profound deficiency was found and then corrected appeared to have the greatest effect on neonatal growth indices. In a recent systematic review and meta-analysis by Thorne-Lyman and Fawzi17 that assessed the association between vitamin D status during pregnancy and maternal, neonatal and infant health outcomes, there was suggestion that vitamin D has a protective effect on low birth weight (three trials, risk ratio (RR) =0.40 [95% confidence interval [CI] 0.23, 0.71]). There was a trend where daily supplementation led to fewer small-for-gestational age (SGA) infants, but this did not reach significance. There were only two trials that met criteria for inclusion in the analysis for preterm delivery, and there was no effect noted as a function of vitamin D supplementation. The conclusion was that there remains little evidence from trials to evaluate the effect of vitamin D supplementation during pregnancy on maternal, perinatal and infant health outcomes17. This was the conclusion of a recent meta-analysis by the World Health Organization as well75. Both meta-analyses suggest that more clinical data is necessary to ascertain the true effect of vitamin D on the mother and her developing fetus.
In an attempt to uncover potential effects of vitamin D during pregnancy with a greater sample size and thus power to detect differences, the NICHD48 and Thrasher Research Fund58 vitamin D pregnancy trials’ data were combined and then analyzed on an intent-to-treat basis59. The studies had used a common data dictionary, questionnaires, and vitamin D dispensed from the same lot number. In the combined cohort, there were 110 in the 400 IU group, 201 in the 2000 IU group, and 193 in the 4000 IU group. No differences between groups in baseline 25(OH)D were found; however, delivery and cord blood values were greater in the 4000 IU group (p < 0.0001), an effect that persisted even after controlling for race and study. While maternal supplementation with vitamin D at 2000 and 4000 IU/d during pregnancy improved maternal/neonatal vitamin D status, a greater percent were vitamin D replete throughout pregnancy in the 4000 IU group (p < 0.0001)58. There was a trend where the 4000 IU group had decreased rates of comorbidities of pregnancy. Evidence of risk reduction in infection, preterm labor, and preterm birth was suggestive, requiring additional studies powered for these endpoints.
It is important to note that more than a third of the women in both the NICHD and the Thrasher Research Fund vitamin D pregnancy trials did not take their vitamin D supplement, which impacted the in- tent-to-treat analysis. When the combined datasets were analyzed on the basis of 25(OH)D at various timepoints during pregnancy, there emerged stronger health associations with vitamin D59: After controlling for race and study site, preterm birth and labor were inversely associated with predelivery and mean 25(OH)D, but not baseline 25(OH)D. There was a strong association between comorbidities of pregnancy and final maternal 25(OH)D; an effect that persisted even after controlling for race and study (p = 0.006). Furthermore, for every 10 ng/mL increase in maternal 25(OH)D at delivery resulted in reduced odds of infection and preterm birth without preeclampsia, but these did not reach statistical significance. When the four main comorbidities of pregnancy were combined, for every 10 ng/mL increase in maternal 25(OH)D at delivery, the odds ratio was reduced to 0.84 (p = 0.006). Maternal delivery 25(OH)D was inversely associated with any comorbidity of pregnancy, with fewer events as 25(OH)D increased.
Soheilykhah et al.76, studied varying doses of vitamin D during pregnancy and their effect on insulin resistance. In their initial case-control study, 54 Iranian women with diagnosed gestational diabetes mellitus (GDM) and 39 women with 1 abnormal oral glucose tolerance test (Impaired Glucose Tolerance; IGT) were compared with 111 non-GDM control women in whom GDM was excluded by glucose challenge test. Controls were matched for gestational age, age, and body mass index with both the IGT and GDM groups. Maternal serum 25(OH)D in GDM and IGT groups at 24-28 weeks of gestation were significantly lower than non-GDM controls (p = 0.001); 83% of GDM compared with 71% of controls met the definition of vitamin D deficiency (<20 ng/mL; p = 0.03), and in fact, women with GDM had a 2.7-fold increased risk of significant deficiency defined as 25(OH)D <15 ng/mL) compared with the control group. In comparison, in an observational, cross-sectional study by Whitelaw et al in the UK involving 1467 women, of whom 137 developed gestational diabetes, there was only a weak association between 25(OH)D and fasting plasma glucose but not with fasting insulin, post-challenge glucose. The issue is that 81% of the cohort met the definition of vitamin D deficiency (25(OH)D < 20 ng/ mL) making it difficult to discern those with gestational diabetes with and without vitamin D deficiency. In addition, of the 137 women, 114 women had raised post-challenge glucose only, 6 with raised fasting only and 17 with both being abnormal. It is only with a prospective, interventional trial that the issue of vitamin D’s effect on insulin resistance and the development of gestational diabetes can be properly addressed.
Going beyond the observational trials, Soheilykhah et al.77, again studied the effects of different doses of vitamin D on insulin resistance during pregnancy. Women (n = 120) less than 12 weeks of gestation were randomized into three treatment groups:
Group A: 200 IU vitamin D daily (control group);
Group B: IU vitamin D monthly; and
Group C: 50,000 IU vitamin D every 2 weeks until delivery.
The serum levels of fasting blood sugar (FBS), insulin, calcium and 25(OH)D were measured before and after intervention, and the homeostatic model assessment of insulin resistance (HOMA-IR) as a surrogate measure of insulin resistance. Serum 25(OH)D increased most dramatically in group C from 7.3 to 34.1 ng/ml; to a slightly less extent in group B from 7.3 to 27.2 ng/ml; group A, however, had only a slight increase from 8.3 to 17.7 ng/ml (p < 0.001). The mean differences of insulin and HOMA-IR before and after intervention in groups A and C were significant (p = 0.01, p = 0.02, respectively). The results of this study suggest that supplementation of pregnant women with 50,000 IU vitamin D every 2 weeks improved insulin resistance significantly. This is one of the first reports of how vitamin D administered during pregnancy impacts outcome. What is set into motion during pregnancy continues during lactation. If a mother is vitamin D deficient during pregnancy then her developing fetus will be deficient, and so, too will her newborn infant23,78-81. Neonatal total circulating 25(OH)D at delivery is 0.7-0.8 that of maternal 25(OH)D48,58. The problems of deficiency that manifest during pregnancy become compounded during lactation: as the mother who is providing breast milk to her newborn infant, remains deficient, her breast milk is deficient, and her infant can only receive a certain amount of vitamin D that is far below what is necessary to achieve sufficiency. The stage is set for profound vitamin D deficiency in the infant. In the next section, we discuss these and other issues surrounding vitamin D sufficiency during lactation for both the mother and her breastfeeding infant.Vitamin D Requirements during Lactation For the past three decades, it has been maintained that human milk is “marginally sufficient” in vitamin D necessitating supplementation of breastfed infants2'42'82-84. Initial work on the vitamin D content of human milk first measured only the 25(OH)D moiety, and thus, showed it to be woefully inadequate in vitamin D85. At that time the parent vitamin D could not be measured due to inadequate methodology86,87. The main moiety transferred into breast milk is not 25(OH)D, however, but rather vitamin D itself. The basic problem, though, has been that when studying breast milk, typically there has been little circulating vitamin D in the mothers because they had poor oral intake and limited UV exposure23, impacting on what was measured in the breast milk: when mother herself is vitamin D deficient, there is little vitamin D for transfer into the mother’s milk23'78'79'88. This led to an incorrect premise about human milk as being “marginally sufficient”86, which was corrected only when experiments demonstrating that both UV exposure and increased maternal vitamin D supplementation could produce profound increases in both circulating and milk concentrations of vitamin D but minimal changes in concentrations of 25(OH)D89,90.
Additional insight into the transfer of vitamin D into breast milk came from the work of Greer and Hollis (1984). They studied a hypoparathyroid patient taking 100,000 IU/d vitamin D2 who went through two normal pregnancies and deliveries, and breastfed her infants. Her milk contained nearly 8,000 IU/L of antirachitic activity, mostly as vitamin D2 with relatively little 25(OH)D2 content90. This mother’s milk contained vitamin D2 at 28% of the circulating concentration as compared to 25(OH)D2, which was found at only 1.3% of the circulating concentration90, an observation confirmed in lactating women with “normal” vitamin D status91. Thus, it was clear that the parent compound is transferred from matenal circulation into her breast milk much more efficiently than 25(OH)D. The following relationship has been observed: for every 1,000 IU/d vitamin D3 provided to a lactating woman, about 80 IU/liter will appear in her breast milk45. Thus, to provide 400-500 IU/day for their infants, nursing mothers appear to require 6,000 IU/day of vitamin D3. It was only recently that this premise was test- ed79'80'92. Prior to this NICHD vitamin D lactation trial, recommended intakes for nursing mothers were 400 IU/d and intakes above 2,000 IU/d were considered harmful2. For this reason, for more than a decade, vitamin D supplementation of the breastfeeding infant has been recommended 82,93.
Infant supplementation with 400 IU vitamin D3/day will achieve sufficiency in the vast majority of infants if mother is adherent to supplementation. Maternal supplementation varies by country and by community. In a large US study of infant feeding practices by Perrine et al, adherence to the American Academy of Pediatrics’ recommendation (that all infants receiving less than one liter of formula per day should receive 400 IU/ day vitamin D) fell far below even 20%94. In comparison, adherence among mothers in British Columbia, Canada showed that of the 90% of infants who were receiving breast milk at 2 months of age, 80% were also receiving vitamin D supplementation95. This approach addresses the needs of the breastfeeding infant without taking into account the needs of the lactating mother, nor does it address why maternal milk is “marginally sufficient” or even deficient in vitamin D.
To address the issue of vitamin D sufficiency in both mother and her breastfeeding infant, two vitamin D trials involving lactating women and their infants overseen by Hollis and Wagner78,79 provided pilot data and paved the way for a larger two-site NICHD vitamin D supplementation during lactation trial80,92. The first pilot study was designed to establish vitamin D transfer from the mother to her milk and then to her recipient fully breastfeeding infant. Women were randomized to receive either 1600 or 3600 IU vitamin D2 plus continue to take their prenatal vitamin containing 400 IU vitamin D3 for a total of either 2000 or 4000 IU vitamin D per day. Both mother and infant were followed for three months. It was found that women taking the 4000 IU/day regimen had better vitamin D status, higher milk antirachitic activity, and that their recipient infants had higher 25(OH)D2 concentrations than those in the 2000 IU group. The study confirmed that the vitamin D moiety that passes most freely into breast milk is not 25(OH)D but rather, vitamin D itself. In addition, it was learned that 4000 IU/day vitamin D was not sufficient to achieve adequate vitamin D concentrations in the milk. This led to the second pilot study by our group.
In the second pilot study by Hollis and Wagner et al79, women (n = 19) were randomized to either 400 IU or 6400 IU/day vitamin D3/day. Infants whose mothers were in the 400 IU group received 300 IU vitamin D/day while the infants whose mothers were in the 6400 IU group received placebo. The findings were as predicted: women in the 6400 IU group achieved higher total circulating 25(OH)D concentrations than those in the 400 IU group. Specifically, 6,400 IU/day vitamin D3 safely and significantly increased maternal circulating 25(OH)D and vitamin D from baseline compared to controls (p < 0.0028 and 0.0043, respectively). Mean milk antirachitic activity of mothers receiving 400 IU vitamin D/day decreased to a nadir of 46 IU/L at visit 4 and varied little during the study period (46-79 IU/L) while the mean activity in the 6,400 IU/day group increased from 82 to 873 IU/L (p < 0.0003). Another important finding was that during the fall and winter months with limited sun exposure, an intake of 400 IU/day vitamin D3 did not sustain circulating maternal 25(OH)D, and thus, supplied only extremely limited amounts of vitamin D to the nursing infant via breast milk. The infants did not differ in their vitamin D status: both the vitamin D supplemented infants and those whose sole source of vitamin D was their mothers’ breast milk (the maternal 6400 IU group) achieved similar 25(OH)D concentrations at 4 and 7 months of age. There was no toxicity associated with the higher vitamin D dosing; however, the sample size was small. To ascertain both safety and effectiveness, a two-site comparative effectiveness trial sponsored by NICHD was conducted in 2006-2012. Some studies challenge the concept that maternal vitamin D supplementation should be daily rather than sporadic as a bolus. The main issue with maternal daily dosing is adherence. In some areas of the world, maternal adherence to daily supplements is less than 40%96 and in other areas-greater than 90%95. Bolus dosing has the advantage of being given in a clinic where one can assure 100% adherence. Saadi et al97, first evaluated the effectiveness of daily vitamin D (2000 IU/day) vs. monthly (60,000 IU) in a group of healthy breastfeeding mothers (n = 90) and a group of nulliparous women (n = 88). The mothers and nulliparous women who received daily vs. monthly vitamin D had comparable 25(OH)D by the end of 3-month study period; however, on both dosing schedules, there was persistent, significant vitamin D deficiency noted97. In a follow-up study by the same group98, healthy breastfeeding mothers (n = 90) again were randomized to receive either 2000 IU/day vitamin D2 or monthly boluses of 60,000 IU vitamin D2. All of their infants (n = 92) received 400 IU daily of vitamin D2 for the 3-month study period. Most infants had baseline 25(OH)D <15 ng/mL (< 37.5 nmol/L); however, at the end of the 3-month study period, serum 25(OH)D concentrations had increased significantly from baseline in both groups. Milk antirachitic activity increased from undetectable (< 20 IU/L) to a median of 50.9 IU/L. The authors concluded that combined maternal (either the daily or monthly dosing schedules) and infant daily supplementation was associated with a threefold increase in infant serum 25(OH)D concentrations and a 64% reduction in the prevalence of vitamin D deficiency without causing hypervitaminosis D in either group.
A recent study by Oberhelman et al88, compared a single monthly supplement to a daily maternal supplement in increasing breast milk vitamin D to achieve the endpoint of vitamin D sufficiency in their infants. Exclusively breastfeeding mothers (n = 40) were randomized to receive 5000 IU/d of vitamin D3 for 28 days or 150,000 IU once and were followed prospectively for 28 days. In mothers given daily cholecalciferol, concentrations of serum and breast milk cholecalciferol attained steady concentrations of 18 and 8 ng/mL, respectively, from day 3 through 28. In mothers given the single dose, serum and breast milk cholecalciferol (vitamin D) peaked at 160 and 40 ng/mL, respectively, at day 1 before rapidly declining. Maternal milk and serum cholecalciferol concentrations were related (r = 0.87). Infant mean serum 25(OH)D concentration increased from 16.9 to 39.2 ng/mL in the single-dose group and from 16.3 to 38.7 ng/mL in the daily-dose group (p = 0.88). All infants achieved serum 25(OH)D concentrations of >20 ng/mL. The conclusion of this team of investigators was that either single-dose or daily-dose cholecalciferol supplementation of mothers provided breast milk concentrations that resulted in vitamin D sufficiency in breastfed infants. While the sample size was small and the follow-up was through 28 days, the findings are provocative. Preliminary results from the NICHD two-site vitamin D supplementation during lactation trial suggest that maternal vitamin D supplementation with 6400 IU/ day is safe and effective in achieving vitamin D sufficiency in the exclusively breastfed infant and comparable to what is achieved when an exclusively breastfed infant is receiving 400 IU vitamin D3/ day as a supplement80,92. In this study, 476 mother/ infant dyads were enrolled and randomized into three treatment groups: 206 in the 400 IU group, 71 in 2400 IU group, and 199 in 6400 IU group. 2400 IU group was stopped in 2009 as that treatment failed to increase infant 25(OH)D concentrations resulting in a higher number of infants in that treatment arm with vitamin D deficiency (<20 ng/mL): 31% in the 2400 IU group vs. 6% in 400 IU group and 5% in 6000 IU group. In the two remaining groups (400 IU vs. 6400 IU), maternal vitamin D status at baseline differed by race/ethnicity, education, SES and by latitude, but not by treatment; baseline maternal 25(OH)D concentrations were 29 ng/mL in the 400 IU group vs. 30 ng/mL in the 6400 IU group (p = 0.1). Of the 177 mothers who continued to fully breastfeed through 7 months (n = 83, 400 IU group; n = 94, 6400 IU group), as early as two months into treatment, maternal 25(OH)D differed between the two groups that was sustained to 7-months postpartum (p < 0.0001). As predicted, however, there were no differences in infant 25(OH)D concentration by treatment: 45 ng/mL in the 400 IU groups vs. 43 ng/mL in the 6400 IU group (p = 0.4). No differences in any of the safety measures by treatment (serum calcium, phosphorus, and urinary calcium/creatinine) were noted in the mothers and infants, except in 25(OH)D concentration. Thus, preliminary analyses from this study support the premise that maternal vitamin D supplementation with 6400 IU/day alone safely improved maternal vitamin D status during 6-months of full breastfeeding and was equivalent to maternal/infant vitamin D supplementation of 400 IU/d in achieving infant vitamin D sufficiency. Such findings have implications for vitamin D recommendations for both the mother and her infant during lactation.
Of interest are the factors that predict maternal and infant vitamin D status during lactation. Utilizing the NICHD vitamin D lactation study data described earlier, a series of preliminary separate analyses were undertaken to determine which factors independently predicted maternal and infant vitamin D status in women living at two diverse latitudes: Charleston, SC (32oN) and Rochester, NY (43.2oN)99. In multiple regression models predicting 25(OH)D after controlling for race, insurance status, vitamin D dose at baseline, education, and acute maternal illness during the past month, the factors that were independently positively associated with baseline maternal 25(OH)D were being Caucasian (p < 0.0001), privately insured (p < 0.0001) and summer season (p = 0.0008). When predicting baseline infant 25(OH)D, only season (p < 0.0001) and latitude (p = 0.024) were independently positively associated. At 7 months of lactation, maternal 25(OH)D was positively associated with being Caucasian (p = 0.0051), privately insured (p = 0.037), and with the higher dose of 6400 IU/day (p < 0.0001). At 7 months, infant 25(OH)D was independently associated with race (p = 0.02), but not maternal education, treatment, race, latitude or insurance status. The strongest predictor in both mother and her breastfeeding infant during sustained lactation was maternal supplementation with 6400 IU/ day.
There is compelling evidence that suggests if mother is vitamin D replete and has total circulating 25(OH)D concentrations that are in the range of women who have ample sunlight exposure that her milk antirachitic activity will be sufficient to provide adequate concentrations of vitamin D to her recipient infant, foregoing the need for infant vitamin D supplementation. The work of Hollis and Wagner et al, Saadi et al, and Oberhelman independently support this premise. It is essential that women who choose to breastfeed are aware of their options in achieving vitamin D sufficiency not only for their breastfeeding infants but also for themselves.Summary The vitamin D requirements during pregnancy must take into account the needs not only of the mother but also that of her developing fetus. This relationship continues during lactation such that the mother becomes the sole source of vitamin D for her unsupplemented breastfeeding infant. Whereas in pregnancy, there is a direct relationship between total circulating 25(OH)D and l,25(OH)2D, such a relationship is not seen during lactation or any other time during the lifecycle. To optimize the conversion of 25(OH)D to l,25(OH)2D, a woman should attain a 25(OH)D concentration of at least 40 ng/mL (100 nmol/L) during pregnancy.
The impact of vitamin D deficiency on the health of the pregnant woman and her developing fetus is just beginning to be understood. At the very least, a woman should attain a 25(OH)D concentration that will allow her to have optimal conversion of 1,25(OH)2D, the active hormone that is more than twice the concentration during pregnancy than it is during the nonpregnant state.
It is clear from work conducted during the past three decades that human milk can and is often deficient in vitamin D. This is not because there is something inherently wrong or bad with human milk; rather, it is a reflection of maternal vitamin D status. Mother is the reservoir of vitamin D for her breastfeeding infant; if she is deficient, so too will her infant be deficient. Therefore, during lactation, for a mother to have adequate transfer of vitamin D in her breast milk and thus to her recipient breastfeeding infant, mother should attain a 25(OH)D concentration of at least 45 ng/mL, a concentration consistently and safely achieved on a daily vitamin D supplement of 6000 IU.
While much remains to be learned about vitamin D’s health effects during pregnancy on mother and developing fetus in the short term as well as the long-term, it is reasonable to recommend that no pregnant woman should be vitamin D deficient nor she should have suboptimal 25(OH)D substrate, the essential precursor to 1,25(OH)2D. Similarly, lactating woman should receive adequate vitamin D to ensure that her milk has ample vitamin D for her breastfeeding infant. As more intensive research is conducted to understand vitamin D’s effect on immune function and health, our recommendations will be expanded and refined.
1. 25-hydroxyvitamin D insufficiency in extraskeletal diseasesGrażyna Odrowąż-Sypniewska, Katarzyna Bergmann, Joanna Siódmiak, Aneta Mańkowska-Cyl
Department of Laboratory Medicine, Nicolaus Copernicus University in Torun, Collegium Medicum in Bydgoszcz, Poland
There have been up to now numerous studies showing an association between decreased 25-hydroxyvitamin D levels in the blood and the risks of several extraskeletal complications such as cardiovascular and autoimmune diseases, and cancer.
Aims: The relationship of vitamin D with extraskeletal diseasess is of major interest considering its roles in key biological processes and the high prevalence of vitamin D deficiency worldwide. Most of studies investigating associations between vitamin D and diseases use measurement of a single metabolite 25(OH)D. This short review presents some recent data on vitamin D insufficiency/deficiency in cancer, cardiovascular diseases, obesity, lung diseases and diabetes relating them to our own findings based on the studies performed in patients with ovarian cancer, nontreated hypertension, atopic asthma, subjects with metabolic syndrome and hyperglycemia.
Conclusions:
Understanding of the functions for vitamin D in extraskeletal complications is growing quickly. However, the causal relationships between vitamin D and most extraskeletal diseases are weak. This may be due to the fact that measuring only 25(OH)D will give an incomplete picture that may or may not correlate with function in disease. Therefore continuing further research quantifying the levels of different vitamin D metabolites is necessary to learn more about the real contribution of vitamin D compounds to the pathogenesis of extraskeletal diseases.
The recent systematic reviews and meta-analysis on vitamin D supplementation have shown that there is not enough evidence yet, confirming or ruling out beneficial effects of supplementation.
Until no consensus on vitamin D supplementation is reached it seems reasonable to consider 25(OH)D monitoring to ensure sufficiency.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592
KEY WORDS: ■ EXTRASKELETAL DISEASES ■ VITAMIN D METABOLITES ■ VITAMIN D SUPPLEMENTATION
Introduction
Vitamin D plays a key role in calcium homeostasis however, may also have several extraskeletal effects. The presence of vitamin D receptor (VDR) in different organs such as skin, placenta, pancreas, muscles and in different cells like activated T cells, cardiomy- ocytes, cardiac fibroblasts, vascular smooth muscle cells, vascular endothelial cells and cancer cells led to several efforts aiming elucidation of the role and mechanisms of action of vitamin D in different tissues. The major form of circulating vitamin D in humans is 25(OH)D3 which is hydroxylated to active metabolite l,25(OH)2D3 in the kidney or other tissues. 25-hydroxyvitamin D insufficiency is highly prevalent in general population and presents a serious public health problem1. There are various vitamin D insuficiency manifestations including osteoporosis and propensity to fall, cancer, cardiovascular diseases and hypertension. In addition vitamin D is related to obesity and metabolic syndrome and its concentration is associated with lung function in patients with asthma and chronic obstructive pulmonary disease.
Vitamin D insufficiency and cancer
People exposed to the sunlight seem less likely to develop cancer thus the possible association of circulating 25(OH)D levels with cancer was evaluated in many studies2. Recent reports from the animal models have indicated that active vitamin D metabolite may inhibit cancer progression. It has been suggested that l,25(OH)2D3 may act to inhibit growth of human breast cancer cells3. These findings indicate for the possibilities of new therapies in humans4.
Most of earlier studies concerned the association of vitamin D level with breast, colon and prostate cancer, only a few concerned the association with ovarian cancer. In patients with epithelial ovarian cancer, aged 37-79, who undergone optimal cytoreductive surgery the pre-surgery concentration of serum 25(OH)D3 was measured. Mean level of 25(OH)D3 in women with cancer was in the range of deficiency (l2.5±7.75 ng/mL) and significantly lower than in the age-matched women without cancer5. There was no correlation of serum 25(OH)D3 with clinical features such as histological subtype, grading, FIGO stage and menopausal status. In the subgroup of patients with 25(OH)D3 level over 10 ng/mL overall 5-year survival rate was significantly higher compared to women with severe vitamin D deficiency (concentration below 10 ng/mL). It was concluded that very low 25(OH)D3 concentration associated with lower overall survival rate might suggest for the important role of severe deficiency in more aggressive course of ovarian cancer. Moreover, it was indicated that testing for 25(OH)D in the standard procedure could help to find ovarian cancer patients with worse prognosis, who would benefit of special attention and supplementation5.
In general, no association was reported on the effect of treatment of vitamin D deficiency on the risk for cancer. However, recent recommendations of the US Preventive Services Task Force on the use of vitamin D supplementation for the prevention in populations at high risk of cardiovascular diseases and cancer address supplementation without first determining a vitamin D status6.Vitamin D insufficiency and cardiovascular diseases Vitamin D may play a significant role in the cardiovascular system. Vitamin D receptor was found in cardiomyocytes and cardiac fibroblasts, vascular smooth muscle cells and vascular endothelial cells. Several cardiovascular disorders were associated with insuficient/deficient serum 25(OH)D levels. Interestingly, the mouse model with complete deletion of VDR gene showed hypertension with increased renin concentration and cardiac hypertrophy7. Data from observational, cross-sectional and, most but not all, prospective studies show that low serum 25-hydroxyvitamin D concentration is associated with higher risk of hypertension8'9. The mechanism underlying the inverse association of 25(OH)D concentrations with blood pressure is not well understood and seems to involve not only regulation of renin-angiotensin-aldosterone system but also stimulation of systemic and vascular inflammation, increase of insulin resistance and the expression of the natriuretic peptide receptor10. Epidemiologic and experimental data have suggested that low level of 25(OH)D may lead to vascular smooth muscle cell proliferation, endothelial cell dysfunction, vascular and myocardial cell calcification11. Gardner et al created a mouse with selective deletion of the VDR gene in vascular endothelial cells. They demonstrated that this mouse displayed many features normally associated with endothelial dysfunction12.
Sypniewska et al evaluated the associations of 25(OH)D level with biomarkers of endothelial dysfunction (CRP, ICAM), subclinical organ damage (PWV, IMT) and insulin resistance in adults with newly diagnosed non-treated hypertension13. The study was performed in adults with normal blood pressure and subjects with diagnosed hypertension. Patients were classified based on ambulatory blood pressure (BP) monitoring. In all subjects laboratory assays, echocardiography, pulse wave velocity (PWV), intima- media thickness (IMT), left-ventricular mass (LVM) measurements were performed. Serum 25(OH)D3 was significantly lower in patients with hypertension than in the reference group. In the study group 63.6% had 25(OH)D3 in the range of deficiency (<20 ng/mL), 58.1% had increased PWV, 41.8% insulin resistance. 25-hydroxyvitamin D3 concentration in the study group correlated weakly but significantly with systolic BP (r=-0.39), PWV, IMT (r=-0.33) and diastolic BP (r=-0.26). Multiple linear regression analysis in the hypertensive group has shown that 25(OH)D3 and intercellular adhesion molecule (ICAM) explained 25% of systolic BP variation. 25(OH)D3 and either PWV or IMT explained 21% and 23% of SBP variation. Itwas concluded that the impact of 25(OH)D3 on systolic blood pressure variation, mediated by its effect on endothelial dysfunction and subclinical organ damage, is modest but significant.Vitamin D insufficiency and metabolic syndrome Very interesting is the role of active vitamin D metabolite l,25(OH)2D3 in adipose tissue metabolism4. Vitamin D insufficiency has been found in young women, aged 25-40, with excessive body mass and metabolic syndrome, in addition 25(OH)D3 correlated inversely with insulin resistance and blood pressure [Mankowska-Cyl unpublished study]. It was suggested that vitamin D insufficiency (<30 ng/ mL) can be a predictor of the occurrence of metabolic disturbances in young women with overweight and obesity.
With the use of mouse model the mechanism of vitamin D action on adipocytes was partly elucidated. It was shown that l,25(OH)2D3 induced intracellular calcium ions signal which initiated apoptosis in adipocytes14. These observations, if confirmed in humans, may indicate on the new approach for the treatment of obesity. However the adequate and safe doses of vitamin D and calcium have to be established for obese individuals.Vitamin D insufficiency and pulmonary diseases Vitamin D insufficiency may be associated with respiratory infections and possibly airway remodeling. In epidemiological studies 25-hydroxyvitamin D deficiency was suggested to be related to the development of asthma and the frequency of asthma symptoms15. Vitamin D deficiency may weaken pulmonary defenses against respiratory infections, and this would contribute to the triggering of asthma exacerbations. The evaluation of the relationship between asthma and vitamin D deficiency must take into consideration several aspects, such as the association with increased airway responsiveness, higher eosinophil counts and serum IgE levels, and the potential role of 25(OH)D in airway remodeling. This process occurs early in asthma, as a consequence of the production of mediators and growth factors by inflammatory and resident bronchial cells. The association of airway remodeling with low vitamin D concentrations was observed in severe and therapy-resistant pediatric asthma16'17. As 25(OH)D insufficiency/ deficiency is highly prevalent in pediatric population18,19, we aimed to elucidate the association of serum 25-hydroxyvitamin D level with markers of eosinophilic inflammation and airway remodeling20. The association of serum 25(OH)D with peripheral blood eosinophil counts, serum IgE and periostin (a potential surrogate marker of airway remodeling) was assessed in 110 children, aged 2-12 yrs, with newly diagnosed untreated asthma.
In children with atopic asthma significantly lower 25(OH)D, elevated IgE concentrations, and eosinophil counts were found compared to the age-matched reference group (p<0.0001). Decreased levels of vitamin D (<30 ng/mL) had no effect on eosinophilia in asthmatic children. IgE significantly increased eosinophilia but the effect of periostin was very small though significant. Serum periostin and CRP were higher in 25(OH)D-deficient children with atopic asthma (<20 ng/mL) (p=0.018; p=0.032) compared to the sufficient ones. Multivariate models, including 25(OH)D, CRP, BMI (body mass index), age, and sex, were statistically significant and accounted for 7% of periostin variation in asthmatics. Only 25(OH)D contributed significantly to the models. It was concluded that in children with newly diagnosed atopic asthma 25(OH)D has a small though significant influence on periostin but no direct effect on eosinophilia. Thus vitamin D may be considered to play a role in early airway remodeling in childhood asthma20.
The association between vitamin D and lung function was also assessed in patients with chronic obstructive pulmonary disease (COPD). The prevalence of 25(OH)D3 deficiency (<20 ng/mL) was found to be very high (58%) in COPD patients21. Mean vitamin D concentration and vitamin D level in deficient COPD patients correlated with lung function parameters. Multivariate analysis revealed that vitamin D was independently associated only with two, out of three assessed parameters, forced expiratory volume in 1 sec and diffusing capacity of the lung4. On the basis of these results it was suggested that vitamin D plays a role in the lung pathology of COPD patients.Vitamin D insufficiency and type 2 diabetes In humans vitamin D insufficiency may be related to the risk of type 2 diabetes as the vitamin D receptor was found in pancreatic beta-cells. The inverse relationship between vitamin D level and hyperglycemia was found in several studies22. The evidence, however is lacking, from intervention studies, whether vitamin D directly contributes to the pathogenesis of diabetes and thus may be essential in the prevention and treatment of the disease4.
The predictive value of glycated hemoglobin (HbA1c) as a risk factor for diabetes and cardiovascular disease was evaluated in young normoglycemic subjects in the 3-years follow-up study. The study included 122 non-smoking, non-obese (BMI <30 kg/m2) individuals, aged 25-40 years, with normal fasting glucose (60-99 mg/dl)23. At baseline, mean 25-hy- droxyvitamin D level in the study subjects was in the range of deficiency (12,7-25,4 ng/ml) and was similar after 3 years follow-up period (13,1-25,6 ng/ml). 25-hydroxyvitamin D insufficiency (<30 ng/ml) was very common at baseline and at the end of the study (77,9% and 82,8%). After 3-years follow-up a negative correlation between HbAlc and 25(OH)D was observed (R= -0,28; p=0,002) and this relationship seemed to be stronger in women. When the study group was divided according to HbAlc tertiles, decreased levels of 25(OH)D were observed in subsequent tertiles, the lower 25(OH)D level the higher HbAlc tertile (p=0,04). HbAlc levels >5,3% were significantly associated with increased risk of 25(OH)D deficiency (<20 ng/ml) after 3-years follow-up (OR=2,29; p=0,035). These results indicate the relationship between 25(OH)D concentration and levels of glycemic control, defined by HbAlc concentration, which suggest that 25(OH)D might be a useful parameter in evaluation of cardiometabolic risk in apparently healthy subjects23.Conclusions There have been up to now numerous studies showing an association between decreased 25-hydroxyvi- tamin D levels in the blood and the risks of several ex- traskeletal diseases such as cardiovascular diseases, stroke and cancer. We have presented some recent data on vitamin D insufficiency/deficiency in cancer, cardiovascular diseases, obesity, lung diseases and diabetes relating them to our own findings based on the studies performed in patients with ovarian cancer, nontreated hypertension, atopic asthma, subjects with metabolic syndrome and hyperglycemia. ■TAKE HOME MESSAGES 1. Understanding of the functions for vitamin D in extra- skeletal complications is growing quickly. However, the causal relationships between vitamin D and most extra- skeletal diseases are weak. This may be due to the fact that measuring only 25(OH)D will give an incomplete picture that may or may not correlate with function in disease. Therefore continuing further research quantifying the levels of different vitamin D metabolites is necessary to learn more about the real contribution of vitamin D compounds to the pathogenesis of extraskeletal diseases.
The recent systematic reviews and meta-analysis on vitamin D supplementation have shown that there is not enough evidence yet, confirming or ruling out beneficial effects of supplementation. Until no consensus on vitamin D supplementation is reached it seems reasonable to consider 25(OH)D monitoring to ensure sufficiency.
- Vitamin D and Cardiovascular disorders
Sekib Sokolovic
Cardiology Clinic, University Clinical Center Sarajevo & Medical Faculty Sarajevo, Bosnia and Herzegovina
Introduction: The association between Vitamin D and Cardiovascular diseases has been validated in a Randomized Clinical Trials (RCT). The goal of our study was to evaluate the relationship between vitamin D, osteoporosis and cardiovascular disorders.
Material and Methods: The retrospective/prospective study was designed and cross sectional evaluation of 146 osteoporotic patients was performed. The transthoracic echocardiography was the major diagnostic tool for identification of calcification in a heart and aorta. Vitamin D concentration was detected by the Elecsys and cobs immunoassay analyzers in a sera of patients with referral values from 30,0-50,0 ng/mL.
Results: All 146 osteoporotic patients had atherosclerosis and calcification in a heart and aorta. Total 82% patients had decreased vitamin 25(OH)D concentrations with median 16.9 ng/mL, with an interquartile range 9.6-26.2 ng/mL. Cardiovascular risk factors were present in a majority of patients. Conclusion: Vitamin D definitely play significant role in cardiovascular disorders, particularly in atherosclerosis, calcification of blood vessels and in osteoporosis as well. Vitamin D should be measured in all patients suffering from numerous disorders, particularly with heart and bone involment.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592
KEY WORDS: ■ VITAMIN D ■ OSTEOPOROSIS ■ ATHEROSCLEROSIS ■ CARDIOVASCULAR RISK FACTORS
Introduction
The association between Vitamin D and Cardiovascular diseases has been studied in a numerous RCTs. The evidence based medicine have shown pathophysiological pathways in development of CVDs related to deficient or insufficient vitamin D. This hormone has a great impact on the anticipation of cardiovascular incidents and in the same time on degenerative bone disorders. These patients share the common risk factors. For both disorders, the prevalence of cardiovascular events and osteoporosis increase with age. The objective of this paper was to study the vitamin D and cardiovascular manifestations in osteoporotic patients.THESES This topic is important since vitamin D is not oftenly recognized and monitored in a routine daily clinical practice. particularly its association with a pathophysiology in a development of atherosclerosis and cardiovascular events, from arterial hypertension to coronary and valvular disorders. Since immunity plays extensive role in a numerous diseases, vitamin D as a hormone has significant role in its pathogenesis, but it is still not well accepted by examiners.
Material and method
This study is follow-up of previous retrospective study with new prospective included patients. Total of 146 osteoporotic patients were examined for
FIG. 1 Severe aortic calcification
FIG. 2 Severe Osteoporosis
risk factors and concomitant diseases. Patients with osteoporosis were divided in two groups: The retrospective/prospective clinical study was designed. There were 132 females (90,4%) and 14 males (9,6%). The average age in total was 64,96 years. In the female group the average age was 64,65 years (range 39-90y), while in the male group it was 65,47 years (range 46-78y). The most frequent cause of osteoporosis was Postmenopasal Osteoporosis observed in 75 pts (51,37%) and Glucocorticoid Induced Osteoporosis was observed in 71 pts (48,63%).
The transthoracic echocardiography was performed as the main diagnostic tool for the calcium deposition in the heart and aorta. The cardiovascular risk factor stratification was done in all examined individuals. Data were analysed using MS Office Excel 2010 and SPSS Statistics 21.0, by descriptive and inferential statistical methods. Elecsys Vitamin D total is used for calibrating the quantitative Elecsys Vitamin D total assay reagents on the Elecsys and cobas e immunoassay analyzers. Serum 25(OH) vitamin D in human serum matrix were measured using Rosche Elecsys system on Cobas e 601 analyzers at Clinic for nuclear medicine. Referral values for using this method D vitamin ranges are 30,0-50,0 ng/mL.
Results
All patients with osteoporosis had atherosclerosis manifested in a deposition of calcium in aorta. Majority of patients were females, approximately 65 years old. The arterial hypertension was present in 96 pts, lipids increased in 89 patients, smoking in 82 patients, and 71 pts received glucocorticosteroids. The Vitamin D deficiency was detected in 82%. Median of vitamin D level was 16.9 ng/mL, with an interquartile range 9.6-26.2 ng/mL. (Distribution of vitamin D concentrations in patients is curved (Kolmogorov-Smirnov test), p = 0,000).)
Severe calcification in aortic valve and moderate to severe aortic stenosis in severe osteoporotic in a 74 female patient.Discussion Antihypertensive effects of vitamin D are on the suppression of renin and parathyroid hormone levels, and also has the renoprotective, anti-inflammatory and vasculoprotective properties. It is known that deficient 25(OH)D Vitamin D is an independent risk factor for incident of arterial hypertension1. Physiologic effects of vitamin D is inhibition intimal and medial artery calcification, and mediate the pro-inflammatory cytokine release, adhesion molecule release and proliferation and migration of vascular smooth muscle cells2. The risk factors for the vitamin D deficiency is age 50 or older, darker skin, a northern home, overweight, obese, gastric bypass surgery, milk allergy or lactose intolerance, liver or digestive diseases, Crohn’s disease or celiac disorder. Vitamin D supplementation reduces systolic blood pressure by 2-6 mmHg. For each 10 ng/ml increase in vitamin D levels, 12% lower risk of developing hypertension. People with the highest vitamin D levels had a 30% lower risk of developing HTA compared to the people with the lowest levels3 Another recent study investigated 108173 individuals and examined 35 studies to look at the associations between the allele score
CHART. 2 Severe Spine Osteoporosis: DEXA: -3,26
25(OH)D synthesis score based on variants of genes that affect 25(OH)D synthesis and blood pressure measurement. It was concluded that increased plasma concentrations of 25(OH)D might reduce the risk of hypertension4. A small group of people with hypertension was given 25,000 IU/w of vit D for 8/w. Vitamin D levels increased throughout study. The arterial blood pressure was greatly reduced5. Our study proved hypothesis that vitamin D is associated with cardiovascular disorder.Conclusion The results obtained from our study have shown the link between cardiovascular risk factors, atherosclerosis and osteoporosis in lipid abnormalities, smoking, arterial hypertension, gender and age. Vitamin D deficiency was detected in 82% of the patients respectively. The higher vitamin D levels, the lower arterial blood pressure. ■
1. Endothelial function and pulse wave velocity in patients with chronic heart failure and D-deficiencyAndrei Marhol, Liudmila Yankovskaya
Educational institution „Grodno State Medical University'; Grodno, Belarus
Background: Studies suggest that endothelial dysfunction and vitamin D deficiency play significant role in pathogenesis of chronic heart failure. Association between 25(OH)D in blood plasma and indicators of endothelial function and the elasticity of blood vessels in patients with CHF is not fully disclosed.
Methods: We examined 47 outpatients with CHF of II functional class (FC) by NYNA. Participants were divided into two groups: with optimum level of 25(OH)D in blood plasma and with its deficiency/insufficiency. We assessed vasomotor function (VF) of endothelium, pulse wave velocity (PWV) and level of nitrates/nitrites in blood plasma.
Results: Both groups were comparable in age, anthropometric data, results of the six-minute walk test and blood pressure. The level of 25(OH)D in group I was 39,1 [37,6; 40.3] ng/ml in group II -11,9 [8,6; 14.3] ng/ml (p = 0,00004). The level of nitrite/nitrate in plasma in group II was 13.9 [12.6; 21.7] mol/L, in group I 19.6 [12.6; 21.7] mol/L (p = 0.013). PWV in group I was 9.3 [8.5; 14.1] m/s, the pulse transit time (PTT) - 114.5 [70; 130] ms. In group II PWV was 13.35 [10.1; 16.2] m/s, the average value of PTT - 69.4 [40; 100] ms. Differences between groups were statistically significant (p <0.05). Both groups had positive correlation relationship between the level of 25(OH)D in the blood plasma and PTT value (R = 0,56; p = 0,00067), and negative correlation relationship between the level of 25(OH)D in the blood plasma and PWV value (R = -0,58; p = 0,00032).
Conclusions: Compared to patients with CHF without D deficiency there is a reduction of NO production by the blood vessel's endothelium and an increasing in PWV in patients with CHF in association with deficiency/insufficiency of 25(OH)D in the blood plasma.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592
KEY WORDS: ■ CHRONIC HEART FAILURE ■ VITAMIN D ■ ENDOTHELIUM VASOMOTOR FUNCTION ■ PULSE WAVE VELOCITY ■ NITRATES ■ NITRITES
Introduction
Chronic heart failure (CHF) is the most common complication of cardiovascular diseases with the poorest prognosis and the number of patients with CHF increases from year to year. Only 50-70% of patients stay alive in one year after the development of heart failure and according to the Framingham study the five-year mortality reached 62% among men and 42% among women after establishing of this diagnosis1.
It is known that endothelial dysfunction is part and parcel of the pathogenic mechanism of heart failure. The most widely known substance produced by endothelium is nitric oxide (NO), which metabolic disorders play a major role in endothelial dysfunction. The main initiating factors which cause the reaction of arterial endothelium are the change in velocity of blood flow in relation to endothelial cells and circulating or „intramural” neurohormones. The primary indicator designating the properties of the vascular wall is its flexibility, which reduction in its turn leads to an increasing of systolic blood pressure (SBP) and increasing of pulse pressure. According to epidemiological studies, 60-70% of the elderly persons (over 60 years) have increased rigidity of the vascular wall and increasing of SBP in association with the reduction of diastolic blood pressure (DBP)2.
According to modern concepts, an additional factor contributing to the development of vascular pathology is the deficiency of vitamin D, which receptors are present on the smooth muscle cells and vascular endothelial cells. Available data indicate that most patients with CHF have 25(OH)D levels in the range of insufficiency. One study showed that patients with CHF had 25(OH)D level 34% lower than in a control group of healthy individuals comparable by age and sex. At the same time level of 25(OH)D in the blood plasma of patients with heart failure under the age of 50 years was lower than in those of control group over 50 years3.
However, there is very limited information about the association between 25(OH)D in blood plasma and indicators of endothelial function and the elasticity of blood vessels in patients with CHF.
Aim. Assess the endothelial function and pulse wave velocity (PWV) in patients with CHF with deficiency / insufficiency of vitamin D and without it.
Materials and methods
We examined a total of 47 outpatients with CHF of functional class (FC) II by NYNA that has developed in association with ischemic heart disease and / or arterial hypertension. FC of CHF was determined on the basis of general clinical examination and six-minute walk test. All of the subjects were in a stage of stable CHF without episodes of decompensation during last 3 months. Exclusion criteria were: chronic obstructive pulmonary disease, bronchial asthma, respiratory insufficiency, persistent cardiac arrhythmias, intake of hormonal medicines, insulin-dependent diabetes mellitus, polyneuropathy, cancer.
All patients were divided into two groups depending on the level of vitamin D in the blood plasma. Group I consisted of 25 persons (14 (56%) women, 11 (44%) men) with a level of 25(OH)D in the blood plasma 30 ng/ml or higher, which corresponds to an optimum level.THESES 1. Vitamin D has an effect on the cardiovascular system via an effect on specific receptors located in the myocardium, endothelium, and through effects on the renin-angiotensin system.
- A certain link between vitamin D level and cardiovascular continuum may be suggested.
I#t is important to study the effect of deficiency and insufficiency of vitamin D on endothelial function and vascular wall elasticity as disorder of these parameters are pathogenic mechanisms of chronic heart failure.
Group II consisted of 22 persons (7 (31.8%) women, 15 (68.2%) men) with the level of 25(OH)D in the blood plasma of less than 30 ng/ml, which corresponds to its deficiency/insufficiency. Patients underwent standard anthropometric survey with definition of height, weight and body mass index (BMI).
Assessment of endothelial function was conducted by determining of vasomotor function (VF) of endothelium and the level of nitrates/nitrites in blood plasma. Method of computerised impedancemetry by hardware-software complex „Impekard” on the brachial artery (BA) during the test with reactive hyperemia was used to assess VF of endothelium. Endothelial VF of BA was estimated as the maximum speed of blood filling (dz/dt max) in a percentage ratio to the initial. dz/dt <12% was evaluated as a disorder of the VF of endothelium. By means of the same apparatus we evaluated PWV of the mixed type vessels (carotid-radial artery), which is a criterion of elastic properties of the vascular wall. PWV match the normal rate at a value below 10.2 m/s4.
NO production by the endothelium was evaluated by the total content of nitrate/nitrite in blood plasma by spectrophotometry method using the Griess reagent. Content of 25(OH)D total [25(OH)D2 + 25(OH)D3] in plasma was determined by ELISA using reagents «DRG» (Marburg, Germany).
Statistical analysis of the research results was carried out by means of the application package «STA- TISTICA 7.0». Data is presented as the mean values and standard deviation (M±SD), and in the distribution that is different from normal - as median (Me) and interquartile range [LQ-UQ]. To assess the association between variables correlation analysis by Spearman criterion (R) was applied.
Results
Average age in group I was 62,7±2,9 years, average weight was 87,0±9,0 kg, height - 167±8,6 cm, BMI - 30,9±4,3 kg/m2. Average age in group II was 61,3±6,8 years, average weight was 91,1±14,4 kg, height- 171±11 cm,BMI-30,8±3,5kg/m2.The average six-minute walk test distance in group I was 386,2±32,7 m, in group II - 368,6±40,1 m. Mean SBP in group I and II were 146,1±21,5 and 139, 9±13,4 mm Hg and DBP - 89,4±14,3 and 82,8±8,6 mm Hg, respectively. Thus, both groups were comparable in age, anthropometric data, results of the six-minute walk test and blood pressure. The level of 25(OH)D in group I was 39,1 [37,6; 40.3] ng/ml in group II -11,9 [8,6; 14.3] ng/ml (p = 0,00004).
Mean values of (dz/dt) max were 3.10 [-14; 28] and -5.90% [-24; 9]% in group I and II, respectively. Disorder of endothelial VF was observed in 76% of patients in group I and 81.8% in group II.
The level of nitrite/ nitrate in plasma in group II was 13.9 [12.6; 21.7] mol/L and was lower (p = 0.013) than in group I, where it was 19.6 [12.6; 21.7] mol/L. PWV in group I was 9.3 [8.5; 14.1] m/s, the pulse transit time (PTT) - 114.5 [70; 130] ms. In group II PWV was 13.35 [10.1; 16.2] m/s, the average value of PTT - 69.4 [40; 100] ms. Differences between groups were statistically significant (p < 0.05). Disorder of PWV (> 10.2 m/s) was observed in 48% of patients in group I and 68.2% in group II.
We have established a positive correlation relationship between the level of 25(OH)D in the blood plasma and PTT value (R = 0,56; p = 0,00067), and negative correlation relationship between the level of 25(OH)D in the blood plasma and PWV value (R = -0,58; p = 0,00032) in both groups.Discussion The literature reflects the studies that reveal the mechanism of vitamin D effect on the cardiovascular system through interaction with the immune system, effects on the myocardium and endothelium, on calcium metabolism and on the renin-angiotensin system. In some cases, vitamin D supplementation resulted in a reduction of plasma renin activity, increasing of NO production, lowering of blood pressure5.
We identified statistically significant differences in the level of nitrates/nitrites in blood plasma, which are probably associated with low 25(OH)D levels in blood plasma that have adverse effects on NO production by vascular endothelium.
Restoration of the vitamin D level has a positive effect on endothelial function, reducing the level of serum endothelin-1 and improving the flow-mediated dilation indicators6. Treatment with vitamin D (with a total dose of 600,000 IU of cholecalciferol intramuscularly) was associated with improved endothelial function in patients with coronary artery disease and deficiency/insufficiency of vitamin D7.
Correlations identified in this research emphasize the negative value of the reduced level of vitamin 25(OH)D in blood plasma for the PWV.TAKE HOME MESSAGES 1. Patients with CHF and deficiency/insufficiency of 25(OH)D in blood plasma have worse parameters of NO production and elasticity of blood vessels than those with normal levels of 25(OH)D in the blood plasma.
In both groups of patients with CHF, either with deficiency/ insufficiency of 25(OH)D in blood plasma, or with its normal level, there is a relationship between parameters of elasticity of blood vessels and the level of 25(OH)D in blood plasma.
Assessment of vitamin D supplementation effect on endothelial function and elasticity of blood vessels need to be conducted.
Conclusion
Our findings suggest that there is a reduction of NO production by the endothelium of blood vessels and an increasing in PWV in patients with CHF in the presence of deficiency/insufficiency of 25(OH)D in the blood plasma compared to patients with CHF without D deficiency. ■
1. Vitamin D Insufficiency in Young Children in Russia: the Results of the Multicentre Cohort Study RODNICHOK (2013-2014)I. N. Zakharova1, S. V. Mal'tsev2, T. E. Borovik3, G. V. Yatsyk3, S. I. Malyavskaya4, I. V. Vakhlova5, T. A. Shumatova6, Ye. B. Romantsova7, F. P. Romanyuk8, L. Ya. Klimov9, N. I. Pirozhkova10,
S. M. Kolesnikova11, V. A. Kur'yaninova9, T. M. Tvorogova1, S. V., N.G. Sugian1, Vasil'yeva1,
M. V. Mozzhukhina1, I.D. Maykova1, Ye. A. Yevseeva1, S.I. Lazareva12
Russian Medical Academy of Postgraduate Education, Moscow, Russian Federation
Kazan State Medical Academy, Russian Federation
Research Centre for Children's Health, Moscow, Russian Federation
Northern State Medical University, Arkhangelsk, Russian Federation
Ural State Medical University, Yekaterinburg, Russian Federation
Pacific State Medical University, Vladivostok, Russian Federation
Amur State Medical Academy, Blagoveshchensk, Russian Federation
North-Western State Medical University named after I. I. Mechnikov, Saint Petersburg, Russian Federation
Stavropol State Medical University, Russian Federation
Novosibirsk State Medical University, Russian Federation
Institute for Continuous Training of Health Care Professionals, Khabarovsk, Russian Federation
Children's Outpatient Center 133, Moscow, Russian Federation
This article was originaly published in Voprosy Sovremennoi Pediatrii - Current Paediatrics. 2014;13:30-34
Vitamin D insufficiency is a widespread phenomenon, which has an adverse effect on human health. Some studies shown by now that 30% to 50% of the general population, both in Europe and in the United States, have a vitamin D insufficiency. This problem is also pressing in Russia, which has most of its territory located to the north of the 42nd parallel north and is thus at risk for vitamin D insufficiency. The Russian territory has some areas with decreased insolation and is naturally among the world's regions with a rather high risk of vitamin D insufficiency and deficiency. A pressing problem is to ensure adequate vitamin D levels in children in their 2nd or 3rd year of life whose diet may not contain a sufficient vitamin D amount, whereas insolation-dependent endogenous synthesis of this vitamin is insufficient as well.
Study objective: To evaluate the vitamin D sufficiency in young children and the adequacy of pharmacological treatment / prevention provided for vitamin D insufficiency in various regions of the Russian Federation.
Methods: Infants and children in their first 3 years of life, who had been admitted for in-patient treatment to Russian health care centres, were examined. Blood samples were obtained at study enrollment to determine their plasma 25(OH)D concentrations. The study lasted from November 2013 to October 2014.
Results: 1,230 infants and children aged from 1 month to 3 years were examined. Vitamin D insufficiency (plasma 25(OH)D concentrations in the range of 21 to 29 ng/mL) was detected in 300 subjects (24.4%), and vitamin D deficiency (25(OH)D < 20 ng/mL) in 513 children (41.7%). The prevalence of vitamin D insufficiency and deficiency was independent of the region's geographic location or insolation level.
Conclusion: Over two-thirds of infants and young children in the study sample were found to have a vitamin D insufficiency or deficiency.
It is therefore expedient to revise the current guidelines taking into account the state-of-the-art approaches to the prevention and treatment of vitamin D insufficiency, to make appropriate changes and to implement them in clinical practice.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592
KEY WORDS: ■ YOUNG CHILDREN ■ VITAMIN D ■ INSUFFICIENCY ■ DEFICIENCY ■ RICKETS ■ RODNICHOK STUDY
Background
There has been increasing interest in vitamin D displayed in scientific literature lately. Over 60,000 articles on the subject have been published in the last 50 years. Current research studies are largely focused on the extraskeletal effects of vitamin D1,2. It has been revealed, for instance, that vitamin D deficiency is associated with increased risk of cancer (of the small and large intestines, pancreas, prostate, and breasts)3, diabetes mellitus4, arterial hypertension5, heart failure6-8, peripheral artery disease9, myocardial infarction10, autoimmune and inflammatory diseases, and immune system dysfunctions11'12. Some studies demonstrated a link between vitamin D consumption and decreasing mortality13. It has been acknowledged that all extraskeletal effects of vitamin D in the human body can be ensured by maintaining the concentration of its principal metabolite, 25(OH)D, at levels exceeding 30 ng/mL14-18. It has been shown by now that 30% to 50% of the general population, both in Europe and in the United States, have a vitamin D insufficiency19. This condition is very common in children, because multiple risk factors for its development exist today.THESES 1. Vitamin D insufficiency has an adverse effect on human health.
The Russian territory has some areas with decreased isolation with a rather high risk of vitamin D insufficiency and deficiency.
Proper vitamin D status is essential for toddlers due to rapid growth.
Major factors promoting the development of vitamin D insufficiency in children and adolescents include the following16.
■ Decreased vitamin D consumption or synthesis:
being born to a vitamin D deficient mother;
premature birth;
prolonged exclusive breastfeeding;
dark skin;
_
decreased insolation;
chronic diseases or frequent hospitalizations;
low consumption of foods rich in vitamin D.
Impaired digestion and absorption of nutrients and decreased vitamin D consumption:
coeliac disease;
pancreatic insufficiency (such as in cystic fibrosis);
biliary obstruction (such as in biliary atresia).
Decreased synthesis or increased degradation of 25(OH)D or 1,25(OH)D:
chronic liver or kidney disease;
use of some drugs (rifampicin, isoniazid, anticonvulsants, etc.).
An important task for Russian paediatricians is to evaluate the prevalence of vitamin D insufficiency in children in order to develop modern recommendations for physicians with regard to the prevention and treatment of this condition based on the Russian specifics. The Russian territory has some areas with decreased insolation and is naturally among the world’s regions with a rather high risk of vitamin D insufficiency and deficiency. There are significant differences between the country’s northern and southern regions in the amount of daylight hours and cold times of year when walking outside may be limited, and sometimes unfeasible, for young children.
Another essential factor that has implications for adequate vitamin D levels in breastfed infants is their nutrition. It is well known that breast milk contains small quantities of vitamin D and that vitamin D fortification is one of the key principles in the adaptation of breast milk substitutes. Apparently, the type of feeding (breast- or bottle-feeding) determines the vitamin D level in the body within the first year of life20, and our efforts to increase the proportion of breastfed infants in the absence of vitamin D supplementation may increase the risk of insufficiency or deficiency.
A pressing problem is to ensure adequate vitamin D levels in children in their 2nd or 3rd year of life whose diet may not contain a sufficient vitamin D amount, whereas insolation-dependent endogenous synthesis of this vitamin is insufficient as well. In Russia, unfortunately, in contrast to European countries and the United States, practically no technology exists to fortify children’s and adult foods with vitamin D16. Switching to the “common diet” decreases the child’s vitamin D levels in most cases. The Guidelines “Prevention and treatment of rickets in young children” were issued by the Ministry of Health of the USSR back in 1991. According to these Guidelines, the optimal way to prevent a low vitamin D status in young term infants is daily administration of 400 - 500 IU/day of this vitamin. For Russia’s moderate climate regions, this dose was recommended for autumn, winter, and spring, beginning from the age of 3 to 4 weeks. Specific rickets prevention was not recommended for the period from June to September in view of the “sufficient” insolation during this period. A sunless summer, particularly in the country’s northern regions, could be viewed as an indication for specific prevention in the summer as well. In the presence of risk factors (being born to mothers suffering from obstetric and chronic extragenital diseases, malabsorption syndrome, congenital hepatobiliary disorders, frequent diseases, being born as a twin or shortly after the preceding delivery, early switch to unbalanced bottle-feeding, receiving anticonvulsant therapy), it was recommended to increase the daily dose of vitamin D to 1000-1500 IU for the same time periods and seasons (autumn, winter, and spring, beginning from the age of 3 to 4 weeks). Therapeutic doses of vitamin D were proposed to treat rickets; they exceeded the prophylactic doses 4 to 10 times: 2000 to 5000 IU/day for 30 to 45 days. After a therapeutic effect was achieved, the therapeutic dose was replaced with a prophylactic one, which the child had to receive daily until the age of 2 years and during the winter of the 3rd year of life. At present, however, a sunless summer, living in an ecologically unfavourable region or in the north of Russia, and insufficient exposure to sunlight may be a reason to forgo the summer break and administer the prophylactic dose of vitamin D (500 IU/day) for the summer months as well.
It is impossible to obtain accurate estimates of the prophylactic use of vitamin D in Russian children. No studies have been conducted to assess the vitamin D status in Russian children depending on the region and time of year, age and type of feeding in the first year of life. A need is generally felt to formulate new national recommendations that would reflect the state-of-the-art approaches to the prevention and treatment of vitamin D insufficiency in children. In 2013, the Chair of Paediatrics of the Russian Medical Academy of Postgraduate Education (Moscow) organized and conducted a pharmaco-epidemiologi- cal study titled RODNICHOK (a study to evaluate the vitamin D sufficiency in young children in the Russian Federation and to analyze the pharmacotherapy of vitamin D insufficiency used in general clinical practice), which aimed to assess the vitamin D sufficiency in young children in the Russian Federation and to determine whether the pharmacotherapy/ prevention of vitamin D insufficiency was adequate in different regions of the Russian Federation.
Materials and methods
Study plan (design)
A multicentre, prospective, cohort study.
Inclusion criteria
Children were selected for this study as they were admitted to the participating health centres based on the following inclusion criteria:
age from 1 month to 3 years;
no organic disorders or genetic syndromes;
permanent residents of the regions participating in the project.
The study did not enroll children with an established diagnosis of rickets, hepatic or renal impairment (jaundice, diarrhoea), or mental retardation.
Study setting
To obtain a representative sample, this study enrolled 7 leading regional research centres located in the North-West, Centre, South, Volga Region, Ural, Siberia, and Far East of the Russian Federation. The cities are situated at different latitudes and, accordingly, differ in the amount of sunny days per year. Participating cities included: Naryan-Mar, Arkhangelsk (the city with the lowest annual insolation level in the country), Saint Petersburg, Moscow, Kazan, Stavropol, Yekaterinburg, Vladivostok, Blagoveshchensk, Khabarovsk, and Novosibirsk.
Outcome registration methods
In order to evaluate the vitamin D sufficiency in study subjects, we determined the concentrations of 25-hydroxyvitamin D (25-OH vitamin D) and other hydroxylated metabolites of vitamin D in serum and EDTA- and lithium heparin-treated plasma samples by means of chemiluminescent immunoassay (CLIA) with a LIAISON analyzer. A vitamin D deficiency was diagnosed at plasma 25(OH)D concentrations < 20 ng/mL, and a vitamin D insufficiency at plasma 25(OH)D concentrations in the range of 21 to 29 ng/mL. Serum 25(OH)D levels above 30 ng/mL were considered normal.
Study duration
The laboratory tests were conducted in this study in the period from November 2013 to October 2014.
Statistical analyses
The sample size calculation was based on the number of infants and children aged from 1 month to 3 years who live in the Russian Federation (5.3 million, as of 17 January 2013) and the expected prevalence of vitamin D deficiency and insufficiency (which can be as high as 40% to 50% according to our estimates). This calculation was performed using the online calculator available at www.openepi. com/v37/Menu/OE_Menu.htm (Open Source Epidemiologic Statistics for Public Health, v. 3.01, updated 2013/04/06). It was determined on the basis of the obtained rate that this epidemiological study had to enroll between 664 and 1,083 subjects).
Results
Study participants
The study included 1,230 infants and children aged from 1 month to 3 years; from 56 to 205 subjects in each city participating in this project.
Principal study results
Only one out of three subjects in the analyzed study sample had a normal 25(OH)D concentration (above 30 ng/mL). Obtained 25(OH)D levels were indicative of a vitamin D insufficiency in 300 children (24.4%) and a deficiency in 513 subjects (41.7%). The prevalence of vitamin D insufficiency and deficiency was independent of the geographic location or insolation level of the respective region (see the Table 1). The highest occurrence of vitamin D deficiency (25(OH)D concentrations < 20 ng/mL) was in Vladivostok (almost in 75% of the children), Kazan (67%), Novosibirsk (65%), and Stavropol (over 45% of the subjects). The lowest
FIG. 1 Vitamin D sufficiency in young children by age
prevalence rates of vitamin D deficiency were registered in Moscow (27%), Yekaterinburg (29%), and Arkhangelsk (30%). Vitamin D insufficiency was found in almost one-third of the children residing in Moscow, Stavropol, Khabarovsk, and Saint Petersburg. Vitamin D insufficiency was somewhat less frequent (approximately 1 out of 5 subjects) in Yekaterinburg and Arkhangelsk.
Additional study results
Our analysis of the vitamin D sufficiency in infants and children of different ages demonstrated that 60% of infants aged from 6 to 12 months, less
than 30 % of children aged between 1 and 2 years, and only 13 % of children from 2 to 3 years of age had a normal 25(OH)D concentration (> 30 ng/mL)
(Figure 1).
Figure 2 presents the distribution pattern of study subjects with normal vitamin D content depending on the month during which the blood sample was collected for the laboratory test. The greatest number of children with sufficient 25(OH)D concentrations (44%) was registered in subjects enrolled in July, and the lowest (28% to 29%) in subjects included in October, December, and April.
FIG. 2 Numbers of children with normal (> 30 ng/mL) 25(OH)D content by month
Discussion
This study revealed vitamin D deficiency or insufficiency in more than two-thirds of the enrolled study subjects in all participating regions of the Russian Federation. The highest prevalence of vitamin D deficiency was documented in Vladivostok, Kazan, and Novosibirsk children, and the lowest in subjects residing in Moscow, Yekaterinburg, and Arkhangelsk. Despite the measures to prevent vitamin D insufficiency and rickets in infants under one year of age being popular in Russia, a low vitamin D status was found in 61% of infants aged 1 to 6 months and in 40% of infants 6 to 12 months of age. These data may be indicative of a poor efficacy of the currently used prophylactic measures. A similar Canadian study demonstrated that the prevalence of vitamin D deficiency was the highest in children in their 2nd year of life21. These findings thus imply that parents pay more attention to the prevention of rickets in breastfed infants while the recommendations for children aged over one year are not always followed. In addition to the above, the AAP recommends that the prevention of hypovitaminosis D should be initiated from the very first days rather than from the second month of life irrespective of the type of feeding22. This, however, may prove insufficient. Zeghoud et al. demonstrated that only 1,000 IU/ day (rather than 500 IU/day) of ergocalciferol given for one month can normalize PTH concentrations in children with subclinical vitamin D deficiency23.
A study of seasonal serum 25(OH)D variability revealed a high prevalence of low vitamin D status at all times of year. Even in the summer months, normal vitamin D concentrations were determined only in 33% to 44% of examined children.
Limitations of the study
This study was conducted in subjects admitted for in-patient treatment, and therefore, children not requiring treatment for any disease were not included. It is therefore impossible to assess the impact of acute disease or exacerbation of a chronic disease on vitamin D levels in patients.Conclusion As a low vitamin D status is a widespread condition in young children today, vitamin D supplementation is necessary. In accordance with the currently active Guidelines (1991), the vitamin D recommended dietary allowance in Russia is 400 IU24. In view of the results we obtained in this study, the outdated dose recommendations should be revised and National recommendations for the prevention of vitamin D insufficiency in children in Russia formulated based on scientific evidence. Prophylactic use of vitamin D during the summer should be recommended for young children residing in different regions of the Russian Federation, while the vitamin D doses administered during autumn, winter, and spring should be increased depending on regional specifics. The inadequacy of the currently adopted measures to prevent vitamin D insufficiency in young children shows the need to revise the current guidelines taking into account the state-of-the-art approaches to the prevention and treatment of vitamin D insufficiency, to make appropriate changes and to implement them in clinical practice.TAKE HOME MESSAGES 1. Vitamin D deficiency is associated with increased risk of cancer (of the small and large intestines, pancreas, prostate, and breasts), diabetes mellitus, arterial hypertension, heart failure, peripheral artery disease, myocardial infarction, autoimmune and inflammatory diseases, and immune system dysfunctions.
The prevalence of vitamin D insufficiency and deficiency was independent of the geographic location or isolation level of the respective region.
The prevalence of vitamin D deficiency was the highest in children in their 2nd year of life.
Serum 25(OH)D variability revealed a high prevalence of low vitamin D status at all times of year.
- Vitamin D status in residents of Belarus: analysis of the three-year data
E. Rudenka1, A. Rudenka2, O. Kastrytskaya3
Belarusian State Medical University, Chair of Cardiology and Internal Diseases, Minsk, Belarus
Belarusian Medical Academy of Postgraduate Education, Chair of Cardiology and Rheumatology, Minsk, Belarus
FLLC Synevo Belarus
Background: Hypovitaminosis D is a common condition in many regions that has a significant impact on health in individuals of any age but particularly in the elderly.
Methods: The results of the 5185 laboratory measurements of the serum content of total vitamin D, performed in adult persons living in Belarus for the period from January 2013 till the middle of 2015, were analyzed according to gender, age group, year and season.
Results: There was noted annual increase in the number of laboratory studies concerning vitamin D testing: from 1525 in 2013 till 1465 for only the first half of 2015. There were no statistically significant differences in the content of total vitamin D between groups for the surveyed period. The prevalence of vitamin D deficiency in adult residents of Belarus is very high and in the autumn-winter period is more than 50% for all age groups.
Conclusion: The annual prevalence of vitamin D deficiency in adult residents of Belarus for the surveyed period is extremely high irrespective of age, gender and season. Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592 KEY WORDS: ■ VITAMIN D ■ DEFICIENCY ■ RISK FACTORS ■ REGION OF RESIDENCE
Introduction
Currently, deficiency of vitamin D is considered to be one of the worldwide recognized health problems, which is quite common among all categories of the population, especially in elderly people and has serious impact on health1-4'6'7'9-15. Among main causes of high incidence of vitamin D deficiency are adverse environmental, geographic and climatic conditions, global demographic changes, individual factors (national style of dress, use of sunscreens, lifestyle, presence of some diseases etc.) as well as underestimation of the fact that the main source of vitamin D for humans is its synthesis in skin under the influence of effective sunlight as its content in foods is extremely low, so an important risk factor
for vitamin D deficiency is a region of residence5,8. Residents of Belarus are at high risk of vitamin D deficiency due to geographical and climatic conditions16.
The aim of our study was to determine the prevalence of vitamin D deficiency among Belarusian adult population and its dynamics for the period 2013-2015.
Materials and methods
We analyzed data of the laboratory results of the serum content of total vitamin D (25(OH)D) which were performed in our republic in persons aged over 20 years from January 2013 to July 2015. In general 5185 results, obtained from 4 laboratories situated in different regions of the country, were analyzed. Serum content of total vitamin D was determined by electrochemiluminescence protein binding assay technology using Cobas e411 immunoassay analyzer (Roche Diagnostic, Germany) and original reactants Roche Diagnostics GmbH. Morning fasting blood sampling was carried out from the cubital vein in Vacutainer serum tubes, without the addition of preservatives and anticoagulants. After separation of the clot from tube walls by clean dry glass rod the tubes was subjected to centrifugation at a rotation speed of 3000 rev/min for 10 minutes, then the serum was separated and placed in disposable plastic 1,5 ml Eppendorf tubes. Tubes were frozen at temperature -22° C and stored for not more than one month, with a gradual thawing at room temperature prior to performing the analysis. Before setting up the samples the work of the analyzer was tested using appropriate to the party and reagent lot calibrators. Internal quality control was carried out with the appropriate serum (Elecsys PreciControl Bone 1, 2 and 3). According to international recommendations vitamin D levels considered to be normal when values of 25(OH)D exceeded the meaning 30 ng/ml, showings from 20 to 29 ng/ml were determined as insufficiency, less than 20 ng/ml - as deficiency of vitamin D. Statistical analysis was performed using the software package Statisti- ca 6.0. Results of the study are presented as mean values with corresponding parameters of standard deviation (SD). Statistical significance of differences between samples was evaluated by parametric statistics using analysis of variance in the module of factorial ANOVA.THESES 1. Identifying individuals with the presence of hypovitami- nosis D is essential for early and comprehensive prevention of many diseases, including such socially significant as osteoporosis, myopathy of various origins, cognitive impairment in the elderly.
Residents of Belarus are at high risk of vitamin D deficiency primarily due to climatic and geographical features: located on the 53 00' latitude, the country has moderately continental climate with low duration of daylight during autumn and winter, and high cloudiness, which reaches 85% of the daytime in the autumn-winter period, and 40 - 60% in spring and summer, snow can be expected from December to March, and occasionally to April. All this factors significantly reduce the access of UV radiation to the skin.
Elderly people living in Belarus include particular risk group for vitamin D deficiency, because above mentioned factors they have additional ones such as the lack of sun exposure, wearing clothing that covers most of the body surface, low intake of vitamin D reach foods, the presence of concomitant diseases, age-related decline of the skin ability to synthesize vitamin D precursors.
The level of probability of faultless prognosis was set at 95% (the difference between samples were considered statistically significant at p < 0.05). Figure 1 demonstrates the annual frequency of general measurements of 25(OH)D in men and women during the observed period.
All the obtained results were divided into groups according to gender and age group as presented in Table 1.
Results
In order to perform further analysis the obtained results were graded by groups according to year, season, age group and gender (Tables 2 and 3).
The evaluation of differences between samples performed using analysis of variance in the module of factorial ANOVA revealed statistically significant changes in the annual dynamics of 25(OH)D levels within age groups (Figures 2-5).
The next step of the analysis was evaluating the proportion of persons with normal levels of total vitamin D and those with vitamin D deficiency (i.e. levels of 25(OH)D < 30 ng/ml) in each age group according to gender and season (Table 4).
Discussion
According to the analyzed data there was noted tendency in annual decreasing of mean levels of 25(OH)D for the observed period in all seasons in women of age groups less than 40 and 41-60 years and in men of all age groups in winter and age group <40
FIG. 2 Annual dynamics of 25(OH)D levels in autumn FIG. 3 Annual dynamics of 25(OH)D levels in spring
and winter in women in accordance with the age group and summer in women in accordance with the age group
-4— <40 41 - 60 —4— >61
FIG. 4 Annual dynamics of 25(OH)D levels in autumn FIG. 5 Annual dynamics of 25(OH)D levels in spring
and winter in men in accordance with the age group and summer in men in accordance with the age group
in summer, though these data were not statistically significant different. Women older 61 years has slightly increased showings of 25(OH)D levels from 2014 to 2015 in both seasons. Unfortunately we couldn’t analyze causes of the presence of risk factors for vitamin D deficiency in studied sample such as the duration of sun exposure, vitamin D supplementation, presence of concomitant pathology, lifestyle etc, but the most likely explanation for positive dynamics of 25(OH)D in women older 61 years is more frequent intake of vitamin D supplements, which are often assigned for prevention or treatment of osteoporosis in women of this age group, either in combination with calcium or not. ■TAKE HOME MESSAGES 1. It was noted the annual increase in the number of laboratory studies performed in Belarus for the observed period in all age groups, which indicates a growing awareness of the problem in the country.
The prevalence of vitamin D deficiency in residents of Belarus is still extremely high irrespective of age, gender and season.
Given the high prevalence of vitamin D deficiency in Belarusian population in combination with adverse geographic and climatic conditions it is necessary to attract attention to this issue both from society and the medical community including government prevention programs.
- Vitamin D deficiency correction in elderly people
V. Povoroznyuk1, V. Muts2, N. Balatska1, N. Dzerovych1, O. Synenky3
D.F. Chebotarev Institute of Gerontology NAMS of Ukraine
Ventiv Health Ukraine, LLC
Lviv Regional Clinical Hospital
Introduction: Vitamin D deficiency and insufficiency are widespread conditions, especially in elderly population with concomitant musculoskeletal disorders. Correction of vitamin D status is crucial to reduce pain, increase mobility and gait stability, and improve overall quality of life in such patients.
Objectives: to assess the efficacy and safety of individual targeted vitamin D therapy in postmenopausal women with skeletal diseases (systemic osteoporosis and osteoarthritis).
Methods: Due to high prevalence of vitamin D deficiency in Ukraine it was developed the individual targeted therapy of vitamin D deficiency. The individual targeted therapy consists of two periods - saturation period and maintenance therapy period, during which patients take it constantly. Duration of saturation therapy is calculated by the formula: Saturation therapy duration (days) = (100 - VDL) x BW/100, where: VDL is blood 25(OH)D level (ng/mL), BW is body weight (kg).
The therapy for saturation includes combined calcium (1000 mg of calcium and 800 IU of vitamin D) and 3000 IU of vitamin D per day. Maintenance therapy includes 2 000 IU of vitamin D per day.
The study involved 70 postmenopausal women aged 46-87 years with skeletal diseases (systemic osteoporosis and osteoarthritis). All subjects were subdivided into two groups: main - 50 women who took individual targeted vitamin D therapy (50 subjects, 65.1±8.8 years old, BMI 27.22±4.51 kg/m2) and control (20 subjects, 64.5±11.1 years old, BMI 26.68±4.95 kg/m2). The duration of the treatment consists of 3 months starting on the 1st Oct 2013. 25(OH)D total and iPTH levels were assessed by electrochemiluminescent method using Elecsys 2010 analytical system (Roche Diagnostics, Germany) and test-systems cobas. The serum levels of calcium, phosphor, alkaline phosphatase levels were evaluated for safety reasons.
Results: In 3 months after the start of the treatment there was a significant (p < 0.001) increase in 25(OH)D levels in the treatment group: 35.60±8.21 nmol/L as compared to baseline levels of 25.20±9.76 nmol/l. Remarkably, the treatment was most effective in the oldest subgroup (> 70 yrs.), as well as in subjects with the BMI 25-28,99 kg/m2. After the treatment, there were no changes in calcium levels.
Conclusions: The suggested individual targeted vitamin D therapy was proven to be effective in postmenopausal women. As the treatment turned out to be effective, relatively quick, and had a reasonable safety profile it may be beneficial for all vitamin D deficient postmenopausal women.
Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 587-592
KEY WORDS: ■ VITAMIN D DEFICIENCY ■ INSUFFICIENCY ■ CORRECTION ■ SCHEME ■ EQUATION
Introduction
Vitamin D administration is widely used in clinical practice as it can be arranged in several formulations and multiple doses - up to 50,000 IU per capsule. However the question remains what would be the correct dose in a given setting to avoid hyper- vitaminosis1'2 but at the same time maintain appropriate treatment effect for extended periods of time3. Previous studies4-6 have shown that it is crucial to maintain long-term and stable serum vitamin D levels in patients with skeletal diseases. It has been suggested that daily administration of 1000 IU of calciferol throughout 3-4 months secures the mean increase in serum 25(OH)D level for about 25 nmol/l. However the pharmacokinetic profile in this case is non-linear and the more pronounced baseline deficiency is the more challenging will be its correction7.
It is also known that the daily vitamin D dose in elderly patients with osteoporosis and osteoarthritis should amount to at least 600-800 IU since the ranges of 400 IU and less exert no therapeutic effect3,8-10. Other sources suggest the need to calculate weekly rather than daily vitamin D dose in this patient population11,12. Either way, there is a consensus regarding the vitamin D dose elderly patients should be receiving in a week - 50,000 IU on average till the mean serum 25(OH)D level reaches at least 30 ng/ml so that the patients may switch to maintenance dose - typically 1,500-2,000 IU daily. It has also been suggested that in such cases patients are to receive booster doses of 50,000 IU every two weeks thereafter despite ongoing maintenance therapy.
When calculating an individual vitamin D dose several factors should be considered. Of special interest is baseline serum 25(OH)D level10, as well as BMI13,14. Indeed, obese patients should be receiving 2-3 times higher calciferol doses to achieve comparable serum 25(OH)D doses to the subjects with normal BMI10,13,14.THESES 1. During vitamin D deficiency correction in elderly patients it is important to consider several factors such as patient's body mass and pre-existing serum 25(OH)D level.
The individual targeted therapy consists of two periods - saturation period and maintenance period: during the latter, patients are getting a steady dose of vitamin D.
The individual targeted vitamin D therapy has been proven to be effective and safe in postmenopausal women.
It has been proven that among elderly subjects, vitamin D deficiency and insufficiency is more prevalent and more pronounced in patients with osteoarthritis and osteoporosis15,16 while these diseases tend to have less favorable prognosis in vitamin D deficiency setting17. At the same time until recently we have seen no well-defined approach to calculating vitamin D dose in such patients.Methods and materials To develop the most suitable vitamin D deficiency correction scheme in this patient population we have enrolled 70 postmenopausal women aged 50-89 years (mean age 65.6±8.4 yrs; mean BMI 26.93±4.57 kg/m2) into the study. All these women had musculoskeletal disorders.
Patients were assigned into either of the 2 treatment arms: main group with 50 women (mean age 65.1±8.8 yrs; mean BMI 27.22±4.51 kg/m2) receiving targeted vitamin D therapy, and control group with 20 women (mean age 64.5±11.1 yrs, BMI 26.68±4.95 kg/m2) receiving placebo.
The study commenced on 1st Oct 2013 and ended on 1st Apr 2014. Main exclusion criteria were as follows: disorders potentially impacting calcium metabolism, intake of steroids, antiepileptic drugs, vitamin D formulations within 6 months prior to study start. Saturation therapy duration was calculated according to the following equation: n=(100 -VDL) x BM/100, where n - duration of saturation therapy in days, VDL - baseline serum 25(OH)D level (ng/ml), BM - body mass, kg.
Study results
Three months after the start of correction therapy, patients had significant serum 25(OH)D level increase (p < 0,001) up to a target level 30-50 ng/ml (according to the existing recommendations for the Central European countries). Subjects enrolled into the control group had no significant changes.
We have analyzed the impact of different factors on the efficacy of treatment. For that purpose, we have assessed the study results across the following age groups: 50-59, 60-69, and over 70 years old.
We have registered significant post-treatment serum 25(OH)D level increase in all age groups. Moreover, the correction turned out to be more effective in older patients group where mean serum 25(OH)D level increased almost 50% compared to baseline.
Apart from subject’s age, another factor influencing baseline vitamin D status and treatment efficacy can be body mass index. We have studied mean serum 25(OH)D level changes after the treatment. The results are noted in Table3
It must be noted that the therapy turned out to be effective in all IMT groups. Compared to baseline, mean serum 25(OH)D level increased by 49% in patients with BMI 25.0-28.9 kg/m2, by 42.1% in those with BMI >29.0 kg/m2 and by 34.8% in subjects with normal BMI. The duration of treatment was the longest in obese patients.
We have also analyzed the efficacy of suggested therapy depending on the baseline serum 25(OH)D level. In subjects with pre-existing vitamin D deficiency baseline levels were registered at 13.42±3.91 ng/ml, while following the therapy administration these rose more than two-fold to 30.68±6.43 ng/ ml. Patients with vitamin D insufficiency (baseline serum 25(OH)D level 24.52±3.26 ng/ml) experienced post-treatment increase up to 36.29±6.11 ng/ml (p < 0.0001).Discussion While the proposed vitamin D deficiency and insufficiency correction scheme was in general effective, we have noticed several important considerations which may help general practitioners to approach individual patients more accurately. In particular, the correction was more effective in older group. This can be explained by worse baseline vitamin D status in people over 70 years old (in this age group, mean serum 25(OH)D level was 20.91±8.36 ng/ml compared to 50-59 years old group (24.99±9.64 ng/ml) as well as 60-69 years old group (28.61±9.86 ng/ml). Then, BMI also had a significant impact on the correction efficacy and the overall duration of therapy. This was expected as it takes longer to saturate internal depots in obese patients.
In general, we have noted that the quickest and most effective correction is expected in subjects with the most pronounced vitamin D deficiency at baseline. Nevertheless the proposed therapy was effective in all patient groups.
FIG. 1 Mean serum 25(OH)D changes in postmenopausal women undergoing targeted vitamin D correction depending on their baseline status (chart A - those with pre-existing vitamin D deficiency, chart B - those with insufficiency)Conclusions To develop an effective scheme of vitamin D deficiency correction in elderly patients, it is important to consider baseline serum 25(OH)D levels, as well as patient’s age and BMI. The suggested equation (n=(100 -VDL) x BM/100, where n - duration of saturation therapy in days, VDL - baseline serum 25(OH)D level (ng/ml), BM - body mass, kg) can be used in clinical practice as it turned out to be effective in various settings. ■TAKE HOME MESSAGES 1. The correction of vitamin D deficiency is most effective in case an individual approach is exercised.
The individual targeted therapy consisting of two periods - saturation period and maintenance therapy period, is an effective method to obtain optimal vitamin D level.
The correction of vitamin D status is most effective in subjects with pre-existing vitamin D deficiency, and the more profound the deficiency is the more beneficial the suggested treatment turns out to be.
Introduction: The numerous evidence showing spectrum of vitamin D effects on human health resulted in the amendment of vitamin D supplementation guidelines, and raised discussion on the risk of hypercalcaemia as a result of the dissemination of novel recommendations. The aim of this study was to analyze the scope of serum 25-hydroxyvitamin D levels change over the last 30 years of activity of a single pediatric clinic.
Materials and methods: Calcium-phosphate metabolism markers and 25(OH)D levels were investigated in a group of 3657 children aged 0-18 years, divided into 2 age groups. Group I consisted of newborns and infants aged 0-18 months (n = 2990; mean age 8.0 ± 3.0 months). The second group consisted of children aged 1.5-18.3 years (n = 667; mean age 8.3 years; 99.1 months ± 63.9).
Results: In neonates and infants (group I) 25(OH)D < 20 ng/ml were noted in 20.2% (n = 605), 20-30 ng/ml in 707 (23.6%) and 30-50 ng/ml in 1067 (35.7%). In group II (1.5-18.3 years) 25(OH)D < 20 ng/ml were found in 270 patients (40.2%), 20-30 ng/ml in 202 (30.1%) and 30-50 ng/ml in 142 patients (21.1%). In group I the mean 25(OH)D was 37,0 ng/ml. In group II, the highest 25(OH)D levels were noted in a subgroup aged 1.5-3 years (35.9 ng/ml). In the following age groups within group II an age-related 25(OH)D level decrease was noted, with a minimum observed at the age 14-15 years (16.59 ng/ml). Severe vitamin D deficiency (25(OH)D < 10 ng/ml) was found in 161 neonates and infants (5.4%) and in 66 patients (9.9%) from group II. In both groups revealing 25(OH)D < 10 ng/ml a normal calcaemia (2.25-2.65 mmol/l) was noted in 82.8% of neonates and infants (n = 134) and in 56 patients (84.8%) in group II. In group I 78 subjects had 25(OH)D above 100 ng/ml, with co-existing calcaemia range: 2.6 mmol/l up to 4.38 mmol/l (mean Ca = 2.70 mmol/l). In group II 9 subjects revealed 25(OH)D above 100 ng/ml, accompanied by calcaemia range: 2.06 mmol/l up to 2.54 mmol/l (mean Ca = 2.35 mmol/l). The prevalence of hypocalcaemia (Ca < 2.25 mmol/l) was a higher in group II (10.1%, n = 68) compared to group I (0.5%, n = 14). In group I 425 patients had Ca levels > 2.65 mmol/l (14.6%). In group II Ca > 2.65 mmol/l were noted in 3.7% (n = 25). In general, the average values calcium-phosphate markers were within the range of reference values for age.
Conclusions: 40.2% of cases from group II, and 20.2% of neonates and infants (group I) revealed a vitamin D deficiency (25(OH)D < 20 ng/ml). Vitamin D supplementation appeared effective in children aged 3 years and younger. A direct relation between low 25(OH)D levels and hypocalcaemia was not observed. Hypercalcaemia concomitant to high 25(OH)D levels (> 100 ng/ml) was reported more frequently in neonates and infants (group I). Standardy Medyczne/Pediatria ■ 2015 ■ T. 12 ■ 112-116
KEY WORDS: ■ VITAMIN D ■ HYPERCALCAEMIA ■ HYPOCALCAEMIA
POSTERS
- Vitamin D status in north-west russian region
Karonova TL12, Nikitina IL1, Popova PV1, Zazerskaya IE1,
Safonva AA3, Kuznezova LV1, Novikova TV1, Galkina OV2,
Vasilieva EYu1, Grineva EN12
North-West Federal Cinical Research Centre, St. Petersburg, Russia
Pavlov First Saint Petersburg State Medical University,
St. Petersburg, Russia
North-West State Medical University of name I.I. Mechnikova, St. Petersburg, Russia
Osoba prezentująca: Tatiana Karonova ([email protected])
Introduction: Russia is a country with geographic and economic preconditions for the development of vitamin D deficiency.
Purpose of work: We analyzed serum 25(OH)D level in residents from North-West region of Russia to study the prevalence of vitamin D deficiency.
Methods: The study population included 2265 (2145 adults 18-75 y.o., including 275 pregnant women and 120 children/adolescents of 3-17 y.o.). Serum 25(OH)D was determined by chemiluminiscentic method on AbbottArchitect 8000, USA. Endocrine Society criteria (2011) were applied. Maternal plasma 25(OH)D concentrations were measured at 8-14 weeks of gestation.
Results: Serum 25(OH)D level was 9,8 - 147,5 nMol/L. Serum 25(OH)D level in women was lower than in men (53,9±0,8 and 67,2±2,2 nMol/L).
Conclusion: This study showed high prevalence of vitamin D deficiency in the population from North-West region of Russia, and the association of low 25(OH)D level with female gender, obesity and muscle mass. ■
1. The ways of vitamin d deficiency correction in ukraineVladyslav Povoroznyuk1, Nataliya Balatska1, Victor Muts2, Omelyan Synenky3
D.F. Chebotarev Institute of Gerontology NAMS of Ukraine
Ventiv Health Ukraine, LLC
Lviv Regional Clinical Hospital
Osoba prezentująca: Vladyslav Povoroznyuk ([email protected])
Introduction: Vitamin D deficiency (VDD) and insufficiency are widespread conditions. Only 4.6% of the Ukrainian citizens were found to have normal 25(OH)D values, whereas 81.8% were diagnosed with VDD. High incidence of vitamin D hypovitaminosis makes doctors to search for the ways of its effective treatment and prevention.
Materials and methods: In cooperation with Ukrainian National University of Food Technologies high-fiber baked bread with a cholecalciferol concentration of 25 gg per 277 g was developed. To study its safety and efficacy in VDD correction, 30 postmenopausal women aged 45-80 years were examined. The study lasted for 21 days.
Likewise, individual targeted therapy of vitamin D deficiency (ITTVD) was developed for correction of VDD. ITTVD consists of two phases - saturation period and maintenance period. The saturation therapy includes combined medication: calcium (1000 mg) and 800 IU of vitamin D and an additional 3000 IU of vitamin D per day. Maintenance therapy includes 2 000 IU of vitamin D per day. To study the efficacy and safety of ITTVD, 70 postmenopausal women aged 46-87 years with skeletal diseases were enrolled.
Serum 25(OH)D level was assessed by elec- trochemiluminescent method (Elecsys 2010). Results: Intake of fortified bread has facilitated a significant increase in serum 25(OH)D levels. The mean level of serum 25(OH)D increased from 14.20±2.60 to 20.05±2.74 ng/ ml (p 3 months of ITTVD leads to a significant. Conclusion: Based upon our results, ITTVD and fortified bread administration can be recommended for vitamin D correction in older age groups. Our ITTVD equation has proven to be effective. ■
A possible implication of vitamin D3 deficiency in placental oxidative stress phenomena and progesterone synthesis leading to preeclampsia
Narcyz Knap, Michal Wozniak, Andrzej T. Slominski,
Magdalena Gorska, Jan Wieruszewski, Michal A. Żmijewski,
Ewa Zabul, Robert Tuckey, Kuban-Jankowska Alicja,
Wieslawa Mickiewicz, Piotr Zabul Osoba prezentująca: Narcyz Knap ([email protected])
Introduction: Placental cytochrome P450scc (side-chain cleavage cytochrome P450; CY- P11A1) is a heme-containing enzyme associated with the inner mitochondrial membrane, and is involved in multiple hydroxylations of vitamin D3. Cytochrome P450scc is also responsible for the synthesis of progesterone which is implicated in the molecular pa- thomechanism of preeclampsia if produced
in excess. Interestingly, arachidonic acid hydroperoxide can be enzymatically converted by cytochrome P450scc contributing to increased oxidative stress which is a metabolic hallmark of preeclampsia.
Purpose of work: The goal of the study was to investigate a role of cytochrome P450scc in oxidative stress generation, and potential consequences for progesteron synthesis in the human placenta. It was also tempting to construct a molecular hypothesis linking vitamin D3 as a natural substrate for the enzyme to the pathomechanism of preeclampsia. Material and methods: The study was performed on the human placental mitochondria as well as JAR trophoblast cells exposed to arachidonic acid hydroperoxide, and thus inducing oxidative stress phenomena in a manner typically observed in the course of preeclampsia. The level of oxidative stress was controlled with a nitroxide derivative TEMPOL.
Results and conclusions: Suicidal self-oxidation of cytochrome P450scc led to structural disintegration of heme contributing to enhancement of oxidative stress phenomena in the mitochondrial and cellular preeclampsia model which was prevented by TEMPOL as a carbon-centered radical scavenger. We postulate that high-dose vitamin D3 treatment might stabilize cytochrome P450scc competitively inhibiting free radical generation and excess progesterone synthesis, both of which may contribute to the progression of preeclampsia. ■
1. High-dose vitamin D3 supplementation as a novel strategy in clinical management of wintertime preeclampsiaPiotr Zabul, Michal Wozniak, Andrzej T. Slominski,
Krzysztof Preis, Michal A. Zmijewski, Ewa Zabul, Robert Tuckey, Narcyz Knap
Osoba prezentująca: Piotr Zabul ([email protected])
Introduction: Preeclampsia is a complex pathology affecting 2-8% pregnancies worldwide. Clinical symptoms involve arterial hypertension, edema and sometimes proteinuria. Treatment is mostly symptomatic, and in severe cases C-section is necessary to safely terminate pregnancy. A wintertime increase in preeclampsia incidence has been observed in the population of Caucasian women of Northern Europe for years. A molecular mechanism of the disorder has not yet been elucidated, however there is growing evidence of oxidative stress implication.
Purpose of work: A predominant occurrence of preeclampsia in the wintertime brings up a question about a possible vitamin D3 deficiency as a plausible causative factor in the pathomechanism of the disease. Therefore, it seemed of interest to investigate a potential correlation between the total body oxidative stress and plasma levels of 25-hydroxyvitamin D3 [25(OH)D3] as observed in preeclamptic patients.
Material and methods: A prospective clinical study was launched focusing on women presenting with severe preeclampsia in order to measure urinary levels of 15-F2t- -isoprostanes as markers of oxidative stress and vasoconstriction mediators, and plasma levels of 25(OH)D3. In addition to that, a case study was designed to investigate a potential clinical efficacy of high-dose vitamin D3 supplementation in prevention and treatment of preeclampsia in the wintertime.
Results and conclusions: There was no correlation observed between urinary isoprosta- nes and plasma level of vitamin D3. However, both the control and preeclamptic cohort presented with severe vitamin D3 deficiency. Preliminary results suggest that high-dose supplementation with vitamin D3 be a rational, safe and effective clinical approach in the management of preeclampsia. ■
1. Association of BsmI polymorphism of VDR gene with vitamin D status in children with vitamin D - deficient ricketsNadia Tokarchuk, Maryna Pugach
Osoba prezentująca: Nadia Tokarchuk ([email protected])
Introduction: At present the role of the gene encoding the vitamin D receptor (VDR) isa ctively studied.
Objective: To analyze the impact of BsmI polymorphism of VDR gene on vitamin D status in children with vitamin D-deficient rickets.
Materials and methods: The study involved 120 children aged from 3 to 12 months who had vitamin D - deficient rickets. Polymorphic variants of VDR gene were determined by PCR-RLFP. The contents of 25(OH)D in blood serum was determined using electrohemi-fluorescent method.
Results: Genotype characteristics of polymorphic marker BsmI of VDR gene in children with vitamin D - deficient rickets showed that in the structure of the disease heterozygotes Bb prevailed - 53 people (44,16±4,53)%. While homozygotes of mutant allele B were the lowest proportion - 22 children (18,33±3,53)% with respect to the frequency of heterozygotes (p However, with BB genotype the frequency of vitamin D deficiency was the highest (68,18±10,16)% in children with rickets with accurate relative percent difference between individuals with the same status with bb genotype (35,56±7,13%, p The value of serum 25(OH)D were the lowest in homozygotes of mutant allele B (21,3±3,11 ng/ml) and significantly differed from those in heterozygotes (29,82±2,17 ng/ml).
Conclusion: The dependence between polymorphic marker BsmI of VDR gene and the vitamin D status in infants with rickets was determined. ■
1. Vitamin D levels may influence microarchitecture of bone tissue in menMario Rui Mascarenhas1, Ana Paula Barbosa1, Didier Hans2,
Manuel Bicho3
Endocrinology, Diabetes & Metabolism, Lisbon's Faculty of Medicine, Santa Maria University Hospital - CHLN,EPE, Lisboa, Portugal
Lausanne University Hospital, Lausanne, Switzerland
Genetic Laboratory, Lisbon's Medical School, Lisboa, Portugal
The vitamin D levels and BMD decline with age. Inadequate vitamin D levels may be associated to the high prevalence of osteoporosis and low vitamin D concentration may be related to an increased falls number and subsequent fragility fractures among older persons. Despite the use of DXA and other fracture clinical risk factors, many older people are at risk for fractures, as the BMD does not provide total info on bone strength; The TBS (trabecular bone score), a recent diagnostic tool used to supplement DXA, may allow to estimate bone microarchitectural texture or bone quality; together, TBS and DXA may evidence the strength of bone, determined by material composition and configuration. The role of microarchitecture of bone tissue in relation to vitamin D and PTH is relatively unknown.
Objectives: To evaluate the influence of the blood vitamin D concentrations on the BMD at L1-L4 and the TBS at the spine in men. Material and Methods: The BMD (g/cm2) and the BMC (g) at the L1-L4 in a group of 54 ambulatory men, mean age 56.4 (±12.1) years, were evaluated by DXA and the spine TBS was derived from each spine DXA scan. The blood 25(OH)D3 (ng/ml), osteocalcin (ng/ml) and iPTH (pg/ml) levels were measured. BMI was also calculated (kg/m2). Adequate statistical tests were used. Results: The means (±SD) obtained in men were: L1-L4 TBS = 1.323 (±0.1), BMC = 68.0 (±12.3) and BMD = 1.041 (±0.1), 25(OH)D3 = 20.4 (±9.6), iPTH = 54,3 (±34.3) and osteocalcin = 18.0 (±6.0).
In this group of men, significant correlation coefficients were detected between the blood 25(OH)D3 levels with the BMI, the spine TBS and the osteocalcin concentrations, but not with the BMC and the BMD at the L1-L4. Conclusions: The vitamin D3 may play an important role on the bone quality, as normal men and post-menopausal women with low 25(OH)D3 may have worse bone quality and it is possible that PTH may also act negatively in the bone quality.
Further studies are needed on a larger cohort and it might be worth to investigate also men with osteomalacia. ■
1. Ameliorative effect of vitamin D3 against liver disorders and impaired bone remodeling associated with experimental type 1 diabetesIhor Shymanskyy, Dmytro Labudzynskyi, Anna Mazanova, Mykola Veliky
O.V. Palladin Institute of Biochmistry, National Academy of Science of Ukraine, Kyiv Osoba prezentująca: Ihor Shymanskyy ([email protected])
Introduction: Growing evidence suggests that vitamin D3 (D3) deficiency, systemic inflammation and oxidative stress can activate bone resorption and reduce bone mineral density in diabetes. Liver is thought to play a key role both in D3 metabolism and in initiating and propagating the systemic inflammatory response.
Purpose of work: The study was performed to evaluate the association between the prooxidant and proinflammatory state of the liver, 25-hydroxyvitamin D3 [25(OH)D3] for
mation and bone resorption in STZ-induced diabetes in C56Bl/J6 mice and to assess the effects of D3 treatment (15 IU/mouse per os, for 8 weeks).
Material and Methods: ROS/NO production was determined by flow cytometry with DCF-DA and DAF-DA respectively. Levels of cytochromes, 3-nitrotyrosine and inflammation markers were measured by Western-blot analysis. 25(OH)D3 content in serum was assayed by ELISA. Results. Diabetes was shown to be associated with a decrease in the content of serum 25(OH)D3 (by 40%) and changes in the expression of the major isoforms of D3 hydroxylating enzymes in liver tissue (CYP27A1, CYP2R1, and CYP27B1). Oxidative/nitrosative stress markers and pro-inflammatory factors (phosphorylated p65 subunit of NF-kB, iNOS, VEGF) were found to be elevated in liver. Diabetes reduced osteoprotegerin and increased RANKL levels in serum, indicating the prevalence of bone resorption over osteosynthesis. D3 caused partial normalization of markers of liver oxida- tive/nitrosative stress and inflammation that correlated with better 25(OH)D3 synthesis and improved bone formation/resorption. Conclusions: Our findings can be considered as an experimental substantiation for the efficacy of D3 in the prevention/correction of metabolic changes and impairments of bone remodeling associated with type 1 diabetes. ■
1. Vitamin D status and inflammation in COPD patients: preliminary findings from a seasonal observation studyEmma Carson, Kirsty Pourshahidi, Francina Baldrick, JJ Strain, Martin Kelly, Sharon Madigan, Eamon Laird, Maria S. Mulhern Osoba prezentująca: Emma Carson ([email protected])
Introduction: Chronic Obstructive Pulmonary Disease (COPD) is a disease characterised by chronic airway inflammation and airflow limitation. Vitamin D has been reported to modulate immune function from a T-helper (Th)-1 cell (pro-inflammatory) to a Th-2 (anti-inflammatory) cell profile.
Purpose of work: To investigate seasonal changes in vitamin D status and associated changes in circulating inflammatory markers in COPD patients.
Materials and Methods: COPD patients (n 39) were sampled at the end of winter and the end of summer; the nadir and peak of vitamin D status, respectively. Serum 25-hy- droxyvitamin D [25(OH)D], as a measure of vitamin D status, was quantified using LC-MS/ MS (API 4000, AB SCIEX). A panel of pro- and anti-inflammatory markers were measured in plasma samples using an antibody-based multi-spot assay system (Meso Scale Discovery, MD, USA).
Results: Vitamin D status and plasma concentrations of the pro-inflammatory cytokines, interleukin (IL)-2, IL-8 and tumour necrosis factor-alpha (TNF-a), were significantly higher at the end of summer compared to the end of winter.
Conclusions: Despite a higher vitamin D status at the end of summer, concentrations of some circulating pro-inflammatory cytokines were also higher at the end of summer, contrary to expectation. Nonetheless, these cytokines were not correlated with vitamin D status, which suggests that other confounding factors play a role in immune modulation in COPD patients. This preliminary analysis remains to be confirmed in a sufficiently powered sample size. ■
1. Effect of a primary prevention program incorporating vitamin and mineral supplementation on glycemic status: an observational studySamantha M. Kimball, JC Herbert Emery, Daniel J. Dutton, Jennifer D. Zwicker, Richard Z. Lewanczuk Osoba prezentująca: Richard Z. Lewanczuk ([email protected])
Vitamin D may play a preventive role in type 2 diabetes. Biologically, the active metabolite of vitamin D positively influences insulin secretion and studies report an inverse association between vitamin D status and risk of diabetes, suggesting that vitamin D influences glycemic control. Other micronutrients have been similarly implicated in diabetes prevention. We characterized the effect of a vitamin D3 - centric nutritional supplementation program on glycemic status in a convenience sample.
To determine if optimizing Vitamin D3 status in combination with a multivitamin and Omega-3's effected glycemic status. Participants (n = 1,018) in a prevention program received vitamin D3 alone (Vital 1) or with other supplements (Vital 2). Changes in 25-hydroxyvitmain D [25(OH)D], hs-CRP, hemoglobin A1c (HbA1c) and glycemic status were characterized over one and two years. HbA1 c and hs-CRP were significantly reduced in Vital 2. Having higher 25(OH)D after one year in the program was associated with larger decreases in HbA1c and hs-CRP in Vital 2. There was no change in Vital 1 participants. Normoglycemic participants who progressed to prediabetes/diabetes were 8% in Vital 2 and 16% in Vital 1 at one year. Prediabetic/ diabetic participants at baseline who regressed to normoglycemia were 44% in Vital 2 and 8% in Vital 1 at one year. Comparison across the cohorts suggests that half of the improvement in biomarkers and glycemic status is attributable to vitamin D3.
Dietary supplements reduced the risk of progression to type 2 diabetes and increased the rate of reversion to normoglycemia in high risk participants. A vitamin and mineral supplementation strategy offers a safe, simple and effective management method for improving glycemic status in patients with prediabetes. ■
1. Vitamin D supplementation - positive effects on lipid profile in patients with hypertensionLiudmila Yankouskaya
Grodno State Medical University
Osoba prezentująca: Liudmila Yankouskaya ([email protected])
The aim of study was to assess the effects of vitamin D supplementation on lipid profile in patients with arterial hypertension (AH). Randomized, prospective, cohort, singlecenter study of 104 individuals with stage II AH (50.9±7.3years) was performed. Duration of the follow-up was 15.96±1.7 months. 38 individuals didn't receive cholecalciferol, 66 received it at the daily dose of 2000 IU for 4.4±2.2 months. Serum level of 25(OH)D total (ng/ml) was determined by the immu-noenzymatic assay. Spectrophotometric method assessed total cholesterol (TC), triglycerides (TG), lipoproteins of high (HDL) and low (LDL) density. Atherogenic index (AI) was calculated. Apoliprotein A1 (Apo A1), apoliprotein B (Apo B) were estimated by immunoturbidimetric assay. Apo B/Apo A1 ratio was calculated. Statistical analysis was done using «STATISTICA 10.0».
Results: Baseline level of 25(OH)D total was 25,85[16,8;34,79]ng/ml, at the end of follow-up - 42,11[33,78;54,9]ng/ml. In cholecalciferol group 25(OH)D level was 53,5 [41,3; 68,4]
ng/ml and positively correlated with HDL (R = 0.42; p = 0.01), ApoA1 (R = 0.45; p = 0.006) and negatively correlated with LDL (R = -0.36; p = 0.03), Apo B/Apo A1 ratio (R = -0.36; p= 0.03), AI (R = -0.43; p = 0.008). Dynamics of 25(OH)D positively correlated with HDL (R = 0.36; p = 0.03), ApoA1 (R = 0.48; p = 0.003) and negatively correlated with AI (R = -0.34; p = 0.04). By means of regression analysis we determined that intake of cholecalciferol and stably high level of serum 25(OH)D positively correlated (p Thus, intake of cholecalciferol and stably high level of serum 25(OH)D have a positive effect on lipid profile in patients with AH. ■
1. The Effects of a Preventive Health Program and Vitamin D Status on Metabolic SyndromeJohn Paul Ekwaru, Paul J. Veugelers
Osoba prezentująca: Paul J. Veugelers ([email protected])
We investigated the effect of temporal changes in serum 25-hydroxyvitamin D [25(OH)D] on metabolic syndrome among Canadians enrolled into a preventive health program that promotes vitamin D supplementation. To analyze the effect of increased vitamin D status on the prevalence of metabolic syndrome.
We analyzed longitudinal observations of 6,682 participants with 2 or more study visits between 2007 and 2014. Serum 25(OH)D concentrations were measured at baseline and at subsequent follow-up visits and categorized into 5 categories: ”=125” nanomoles per liter (nmol/L). Metabolic syndrome was identified according to recent harmonized criteria. Logistic regression models were applied to quantify the association of serum 25(OH)D with metabolic syndrome, and the relationship between temporal increases in serum 25(OH)D and metabolic syndrome. At 1 year of follow up participants, on average, had increased their 25(OH)D serum concentrations by 38 nmol/L. We observed a gradient whereby higher 25(OH)D concentrations were associated with a lower prevalence of metabolic syndrome with odds ratios (OR) of 0.21 (95% CI: 0.15-0.28) for women and 0.33 (0.26-0.42) for men with ”>=125 nmol/L” relative to those with ” Improved vitamin D status may help reduce the public health burden for metabolic syndrome, and possible subsequent conditions including type 2 diabetes and cardiovascular disease. ■
1. Serum Vitamin D Status, a Threat neither for Hypercalcemia nor for InflammationNaghmeh Mirhosseini, Ken Fyie, Samantha Kimball
Osoba prezentująca: Naghmeh Mirhosseini ([email protected])
Background: Clinical research suggests that for vitamin D to provide benefit by preventing chronic disease one requires supplementation at doses higher than previously considered. However, the looming risk of toxicity prohibits the use of higher levels of vitamin D supplementation.
Purpose of work: The objective of this study was to characterize the effect of a broad range of serum 25-hydroxyvitamin D concentrations on hypercalcemia and inflammation.
Method: A retrospective, population-based study was conducted on 4,044 Pure North participants with 6-18 months of follow-up in 2012 to 2015. Participants received a wide range of vitamin D supplements (1,000 - 15,000 IU/d). Serum 25(OH)D, calcium, hs-CRP, liver and kidney function tests were measured at the baseline and follow-up visits. Serum calcium was corrected by serum albumin.
Results: Of 4,044 total participants, 13.5%, 3.8% and more than 1% had 25(OH)D values in the ranges of 150-200, 200-250 and > 250 nmol/L, respectively. Hypercalcemia, as defined by albumin-corrected serum calcium > 2.55 mmol/L, was seen in 1.3% of population. Hypercalcemia was not affected by increased serum 25(OH)D. Serum 25(OH)D levels > 300 nmol/L did not affect serum calcium significantly. We also did not find any significant association between serum hs-CRP and 25(OH)D. Moreover, liver and kidney functions were not affected by increased 25(OH)D.
Conclusion: Vitamin D supplementation over a large range of intakes (1,000 - 15,000 IU/d) were found to be safe. Vitamin D intoxication with D3 supplement is a rare condition and hypercalcemia mediated by serum 25(OH)D remains a scarce presentation. Serum 25(OH) D might not be a threat for inflammatory cascade, however obesity was found to be a positive predictor for hypercalcemia and inflammation. ■
1. Synthesis of novel vitamin D analogs and their biological evaluationSharmin Nadkarni
Pharmaceutical Research Institute, Warsaw Osoba prezentująca: Sharmin Nadkarni ([email protected])
The application of vitamin D analogs as an anticancer drugs have been gaining importance over the last few years. Numerous analogs of 1,25(OH)2D3 have been synthesized over the years by several laboratories all over the world. The main purpose of these analogs is to find a potential therapeutic for cancer whilst minimizing or neutralizing the side effects. A large number of double point vitamin D analogs have been synthesized at Pharmaceutical Research Institute (PRI), Warsaw, Poland over the last years. Their biological activities have been studied and a novel strategy had been established for the synthesis of new analogs. Double point modified analogs with elongated side chain which have been synthesized at PRI have shown selective activity. Moreover, this modification in side chain, when coupled with the 19-nor A-ring modification, has been found
synergistic. Hence carrying on the research in the same direction we have synthesized new analogs with elongated side chain, 19- nor modification and an additional C-2 substitution. It was recently noted that the C-2 modification in the A-ring is very beneficial along with the 19-nor modification. Therefore we decided to combine this modification with the elongated side chain which we have developed over the years at PRI aiming for a synergistic effect on the biological profile of the new analogs. For this purpose a synthetic route has been established and the synthesis of new important fragments such as the A-ring, CD-ring and the side chain has been achieved. The coupling of these fragments into the next series of analogs is underway in this laboratory. Apart from this studies we observed that over the years the application of active metabolites of 1,25(OH)2D2 has been underexploited as compared to analogs of 1,25(OH)2D3. There have been no reports by now on the direct comparison of biological activities of 1,25(OH)2D2 and 1,25(OH)2D3. Hence, we synthesized 1,25(OH)2D2 by a novel procedure as well as analogs of thereof [ PRI- 1730, 1731, 1732, 1733 and 1734] for further biological evaluation.
1. Tissue in children with ergocalciferol deficiency in anamnesisTatiana Frolova, Olga Okhapkina, Irina Siniaieva
Osoba prezentująca: Tatiana Frolova ([email protected])
At the modern stage of the society development of osteopoenia (OP) is one of significant problems of paediatrics. Insufficient insolation, non-systemic exposure to fresh air, sedentary lifestyle, and insufficient vitamin D intake from food lead to the formation of vitamin D deficit in children.
Purpose: To establish the character and degree of disorders in the structural and functional state of bone tissue in pupils, who had a history of vitamin D deficiency.
Material and methods: 286 children aged 9-16 years were examined.
Evaluation of structural and functional state of bone tissue (SFS BT) was performed on an ultrasound densitometer. Group I consisted of children with diagnosed rickets (49.65 %). Group II included children without rickets in anamnesis (50.35 %). Statistical analysis of the results was conducted on the basis of the method of stepwise discriminant analysis.
Results and conclusions: The findings demonstrated that (62.1 ± 2.3) % of the children from group I had a reduction in the strength index of their bone tissue, it being significantly higher versus the children from group II (30.4 ± 1.4) % (p < 0.05). The incidence of OP depended on the severity of rickets manifestations (r = 0.67). Data analysis of actual food showed a strong correlation between the level of vitamin D consumption and the bone strength index in pupils (r = 0.75) and a direct correlation of the average strength in adolescents (r = 0.62). Hypovitaminosis D in anamnesis lead to the formation of osteopoenic disorders at school-aged children. This fact should be taken into account during the dynamic observations in this group of patients. ■
1. Correlation between Vitamin D level and Behcet's disease activity in patients in West region of UkraineKhrystyna Lishchuk-Yakymovych, Omelian Synenkyi,
Danylo Halytskyi
Lviv National Medical University
Osoba prezentująca: Khrystyna Lishchuk-Yakymovych ([email protected])
Introduction: Behcet's disease is a chronic inflammatory disease characterized by recurrent orogenital ulcerations, ocular manifestations, arthritis, vasculitis with neurological and large vessel involvement.
Purpose of work: To investigate the correlation between Vitamin D level and Behcet's disease activity in patients in West region of Ukraine.
Material and methods: Ten patients with Behcet's disease and 12 matched healthy controls were enrolled in this study. The erythrocyte sedimentation rate (ESR) and the levels of C-reactiveprotein (CRP), serum 25-hydroxyvitamin D, calcium (Ca), phosphate (P), serum parathyroid hormone (PTH) and TNFa levels were measured in both groups.
Results: There were no significant differences between the two groups regarding demographic data. The serum 25-hydroxyvita- min D levels of patients and controls were 76 and 38.12 ng/ml, respectively. In patients with Behcet's disease, 25-hydroxyvi- tamin D values were significantly lower than those of the healthy controls.
Conclusion: Multivariate regression analysis parameters showed that smoking, frequency of physical activity, use of colchicine and corticosteroids were the main predictors of 25-hydroxyvitamin D levels. Future studies are needed to determine the necessary of vitamin D use in patients with Behcet's disease. ■
1. Dynamics of the vitamin D and of the bone's metabolism other indicators in the pregnant women with perinatal infectionManasova G.S.1, Povoroznyuk V.V.2, Zelinsky A.A.1,
Manasov M.M.3, Kazarenko O.N.4
Odessa State National Medical University
Institute of Gerontology, AMS Ukraine, Ukrainian Scientific-Medical Center of Osteoporosis, Kiev
Health Resort of State Border Service of Ukraine
Maternity home N5, Odessa City
Osoba prezentująca: Vladyslav Povoroznyuk ([email protected])
Introduction: In the infection biochemical and immunological changes in the pregnant independent become, including synthesis and regulation of the bone's metabolism systemic and local factors.
Objective: To study of vitamin's D (VD), some calcium-regulating hormones (CRH), the bone remodeling markers (BRM) levelin the blood of the pregnant women with verified perinatal infection (VPI) and in healthy pregnant women in the gestation's dynamics was.
Materials and Methods: The 3 groups of pregnant women was examined: I-A - the 192 women with osteopenic syndrome and VPI, I-B - 43 women with VPI without osteopenia and II group - 128 healthy women. By the chemiluminescence immunoassay methods the VD level, parathyroid hormone (PTH), calcitonin (CT), osteocalcin (OC) and p-CrossLapsin II and III-trimester determined.
Results: In all groups, there was the gradual decline in VD, at the infection these changes were more pronounced (p < 0.001). PTH activity at infection increased, whereas in healthy women this increase in the III-trimester was significant (p < 0.001). The content CT has increased in the III trimester in both groups, but these changes were more pronounced at infected. In the women with VPI all changes lower was (p < 0.001).The both concentration of OK (p < 0.05) and p-CrossLaps (p < 0.001) levels at infected increased. In healthy women concentration of OK (p < 0.001) decreased, while of p-CrossLaps level (p < 0.01) increased.
Conclusion: In pregnancies complicated by VPI, the VD level in the blood was significantly reduced. The dynamics of the CRH and BRM indicating the activation of the both bones remodeling phases, which as the mechanism aimed to preserving of bone's mineral density inpregnant womencan be considered. ■
1. Vitamin d intakes among pregnant women in an urban and rural population of Western UkraineAlla Boychuk, Tetiana Budnik, Oksana Boyarchuk I. Horbachevsky Ternopil State Medical University,
Ternopil, Ukraine
Osoba prezentująca: Alla Boychuk ([email protected])
Introduction: Vitamin D is important for both mother and child. It prevents pregnancy complications and induce fetal development. Mothers require both sufficient intakes and skin production of this vitamin.
The purpose of work was to estimate the intake and sources of vitamin D in pregnant women from different places of residence (rural and urban) of Ukraine for determining the need of further correction.
Material and methods: The survey of 120 women (60 - rural and 60 - urban) was done. The survey included a questionnaire containing the social block of questions, a block of questions related to the suppliance of vitamin D, as well as questions about the awareness of women recently confined about the role of the vitamin D. A standard questionnaire was used to define the daily intake of vitamin D and calcium from food.
Results: 60 % of the urban women and 30 % of rural women had higher education (X2 = 4.18, p = 0.0408). Majority of urban pregnant women (60 %) and half of rural evaluated their social status as satisfactory, the rest of them - good.
It was found that the average daily intake of vitamin D from food during pregnancy was 301.1 ±59.3 IU in urban and 417.3±72.3 IU in rural women (p 58.3% of the urban and 76.7% of the rural women reported use of vitamin D supplements. 61.7% of urban pregnant and all pregnant from rural areas were outdoor more than 2 hours (x2 = 4.09, p = 0.0431).
Conclusions: Vitamin D intakes from food among pregnant women in an urban population of Western Ukraine is lower than among the rural population. Vitamin D supplementation among pregnant women is necessary for both groups in the period of increased demands. ■
1. The Curious Situation of Europeans and Vitamin D - an Environmental Mismatch?Horst Goring
Osoba prezentująca: Horst Goring ([email protected])
Review: The cradle of Homo sapiens has been in the equatorial high plains of East Africa. There he found necessary and sufficient conditions for his life: readily available food resources, a suitable interval of temperature and high intensity of sun radiation including UV-B radiation. When he migrated to different continents he preferred fertile regions within the range of 20° to 40° of latitude, N and S. There is one exception: Europe. Here people are living in relatively high density at a latitude of 60°N. They were lured here by the moderate climate provided by the warm water of the Gulf Stream. However, at this high latitude only a very low part of UV-B radiation is reaching the earth surface. As a consequence much less cholecalciferol (known as Vitamin D3) can be synthesized in the skin of men. Deficiency in this hormone became an even bigger problem when men changed from being a hunter to becoming a farmer and with all the pressures in his dress code and behavior that civilization imposed at him. Although vitamin D can be acquired to a certain extent through food, it covers only 10-20% of his entire need1. This could not be without consequences for his health. He as a species survived more or less well, but how could the situation be improved for an optimal life of the individual? Are there other regions of environmental mismatch? Vitamin D-deficiency is not only caused by natural conditions, but more and more by social constrains. ■
1. Vitamin D status among healthy infants in Poland - assessment based on randomly selected sample from the populationAnna Stolarczyk, Katarzyna Szott, Paweł Płudowski,
Aldona Wierzbicka, Małgorzata Syczewska, Piotr Socha Children's Memorial Health Institiute, Warsaw, Poland Osoba prezentująca: Anna Stolarczyk ([email protected])
Objective: To assess prevalence of vit. D deficiency among healthy infants in Poland. Methods: Study participants (158 infants aged 6 months and 159 infants aged 12 months) were randomly selected in each of the states of Poland, proportionally to the number of residents and degree of urbanisation. Sampling frame consisted of all citizens of specified age registered by the MSWiA. The study was carried out in March 2011. Data concerning vit. D intake were collected using questionnaire and 1-day food records. 25(OH) D level was assessed in 111 babies aged 6 mo. (70%) and 124 babies aged 12 mo. (78%). Results: Vitamin D intake from diet and supplements was 814 ± 511 IU at 6 mo. and 609 ± 341 IU at 12 mo. of age. The mean vit. D intake expressed per kg of body weight was 103 ± 70 IU at 6 mo. and 59 ± 33 IU at 12 mo. (p and 32.4; p = 0.034).
Conclusions: The prevalence of vitamin D deficiency seems to be high among infants in Poland and increases from with age. 25(OH)D correlates significantly with vitamin D intake. ■
The study was supported by NUTRICIA Foundation.
1. The protective effect of vitamin D3 against prednisolone-induced liver injury in ratsOlga Lisakovska, Ihor Shymanskyy, Anna Khomenko,
Mykola Veliky
Osoba prezentująca: Ihor Shymanskyy ([email protected])
Introduction: Hepatotoxicity has recently been recognized as one of the complications of chronic glucocorticoid (GC) administration.
The development of GC-induced abnormalities can be largely linked to alterations of oxidative metabolism in liver including excessive levels of nitric oxide (NO). Vitamin D3 was shown to be involved in the regulation of impaired oxidative metabolism and detoxifying function of liver.
Purpose of work: The aim of this study was to evaluate the efficacy of vitamin D3 in correcting prednisolone-induced damage to hepatic cells through changes in iNOS/NO system.
Material and methods: Female Wistar rats received prednisolone (5 mg per kg of b.w.) with and without 100 IU of D3 (for 30 days). NO production and cell viability were determined by flow cytometry with DAF-DA and propidium iodide respectively. Levels of inducible NO synthase (iNOS), poly-ADP-ribosylated and nitrated proteins were measured by Western-blot analysis. 25(OH)D3 content in serum was assayed by ELISA.
Results: Prednisolone administration enhanced NO synthesis in isolated hepatocytes, iNOS expression and tyrosine nitration in liver tissue. A marked increase in the level of poly- -ADP-ribosylated proteins was observed and accompanied by 1.7-fold rise in the percentage of necrotic cells among isolated hepato- cytes and a 66% decrease in 25(OH)D3 serum content. Restoration of D3 bioavailability by cholecalciferol treatment counteracted prednisolone effects in liver indicating that D3 deficiency can trigger an oxidative-nitrosative stress-mediated cell death.
Conclusions: Prednisolone-evoked impairment of hepatic function was associated with D3-deficiency and impairment of iNOS/NO responses. Vitamin D3 co-treatment has shown efficacy in diminishing deleterious effects of GC in liver. ■
1. Effect of cholecalciferol on plasma rennin activity in women with arterial hypertension in premenopausal and early postmenopausal periodsLiudmila Kezhun, Liudmila Yankouskaya EE„Grodno State Medical University", Grodno, Belarus Osoba prezentująca: Liudmila Kezhun ([email protected])
Aim: To assess the effect of cholecalciferol on plasma renin activity (PRA) in women with arterial hypertension in premenopausal and early postmenopausal periods who received 25(OH)D supplementation.
Materials and methods: We investigated 102 women with AH stage II risk 3 aged 50[48;53] years: 50 females in premenopausal period - group I and 52 females in early postmenopausal period - group II. PRA and serum level of 25(OH)D were determined by the immunoenzymatic assay. In groups I and II we identified subgroups with the level of 25(OH)D.
Results: By baseline PRA subgroups IA and IB, IIA and IIB did not differ (p > 0.05). The level of 25(OH)D was lower (p 0.05). Significant contribution of cholecalciferol to PRA dynamics was established: F = 6.59, p = 0.01. Conclusion: Correction of 25(OH)D level by intake of cholecalciferol 2000 IU/day for 3 months leads to reduction of PRA in women with AH. ■
1. Multiple mechanisms by which both vitamin D deficiency and toxicity affect cardiovascular healthNaghmeh Mirhosseini, Steven Knaus, Hassan Vatanparast,
Lynn P. Weber
Osoba prezentująca: Naghmeh Mirhosseini ([email protected])
Introduction: Vitamin D supplementation is increasingly being advocated because deficiency is now linked to variety of conditions including systolic hypertension. However, the mechanism(s) by which vitamin D status influences blood pressure are unclear, particularly in toxicity.
Purpose of work: This study aimed to explore the renin-angiotensin system (RAS), inflammation, kidney structure/function and endothelial dysfunction as possible links to hypertension in both vitamin D deficiency and toxicity.
Methods: Normal, male rats were fed diets with different levels of vitamin D [n=14/group; diets with zero, equivalent to human Recommended Dietary Allowance (RDA = 600 IU/d) or toxic vitamin D levels (150,000 IU/d)].
Results: After 4 weeks feeding, systolic blood pressure was increased in deficiency and toxicity compared to RDA (10-15 mmHg). Both vitamin D deficiency and toxicity increased RAS activity compared to the RDA group. Deficiency and toxicity showed kidney histopathology. While vitamin D deficiency showed a tendency for inflammation with increased blood neutrophils, toxicity surprisingly caused more severe inflammation. Finally, vitamin D toxicity, but not deficiency, caused endothelial dysfunction.
Conclusions: Taken together, our findings provide strong evidence that both vitamin D deficiency and toxicity increase RAS activity and inflammation with links to systolic hypertension. However, vitamin D toxicity, previously thought to stem only from hypercalcemia and calcification of soft tissue, activated multiple mechanisms with the potential to cause greater increases in blood pressure. So, looking at probable vitamin D toxicity, inflammation and kidney function should be accounted besides hypercalcemia.
1. The undifferentiated connective tissue dysplasia provide the vitamin D3 for adolescent childrenPochinok T.V., Tyazhka O.V., Zhuravel O.V.
Osoba prezentująca: Olena Zhuravel ([email protected])
Introduction: Nowadays some problems continue to be extremely actual which related to D-hypovitaminosis and disturbance in metabolism in the child's body especially tricaleium phosphate.
Purpose of work: To investigate the level of vitamin D3 in the children with undifferentiated connective tissue dysplasia (UCTD) of juvenile age, by determining the level of 25(OH)D3 venous blood serum.
Patients and Methods: 43 children (21 girls and 22 boys) aged 10 - 16 years: 27 - with NDCTD (13 girls and 15 boys) and 15 children (8 girls and 7 boys) without UCTD determined 25(OH)D3 in the serum of venous blood and hydroxyproline glycosoaminoglycanes in daily urine. A mathematical analysis of the definition of the correlation coefficients was done.
Results: It was found out, that the levels of 25(OH)D3 in the serum of venous blood were significantly reduced in the children with and without UCTD. However, the level of 25(OH)D3 in the children with UCTD was significantly lower (in 81.4% of children with UCTD the level of 25(OH)D3 was below 25 nmol / L) compared with the children without UCTD. Correlation analysis revealed significant inverse relationship between the level of hydroxy- proline and 25(OH)D3, which confirms the hypothesis of impaired synthesis of calcium - binding protein and 25-hydroxycholecalciferol in children with UCTD.
Conclusion: The level of 25(OH)D3 in venous blood serum in the children of juvenile age was significantly reduced. More profound deficiency of vitamin D3 was found in children with UCTD compared with children without UCTD. In order to prevent the development of various physical processes of children of juvenile age, especially with UCTD it is necessary to prescribe vitamin D3 in the autumn-winter period, in conjunction with a balanced diet.
1. Prevalence of 25-Hydroxyvitamin D Deficiency in Children on Dialysis and After Kidney TransplantationBaiko S.V., Sukalo A.V., Rudenko E.V.
Belarusian State Medical University, Minsk, Belarus Osoba prezentująca: Sergey Baiko ([email protected])
Introduction: Vitamin D deficiency is more and more prevalent worldwide whereas current data show that optimal levels should be >30 ng/mL.
Purpose of work: Assess levels of vitamin D, seasonal variations and changes with time in children on dialysis (peritoneal (PD) and hemodialysis (HD), and after kidney transplantation (Tx).
Material and methods: 25-hydroxy
-vitamin D total [25(OH)D] was measured in 107 children (68 boys / 39 girls, age 12.5±4.8 y), all patents were divided in groups: Tx-53, PD -18, HD-24 and control group 12 children with chronic kidney disease 4-5 stage (CKD). In 53 Tx patients assessed independent and in 15 dependent seasonal variations, in 11 Tx - changes with time (winter, 2012/13 and 2014/15 y) without any vitamin D supplementation. A 25(OH)D deficiency was defined by a 25(OH)D level below 20 ng/mL and an insufficiency by a level 20-29 ng/mL. Results: The levels of 25(OH)D among groups (Me (P25;P75) were: Tx 16,8 (13.5; 24.8), PD 13.8 (8; 15,8), HD 17.4 (12.7; 22.3), CKD 24.4 (17.5; 30.1) ng/mL.
Conclusion: Vitamin D deficiency and insufficiency is common in children on renal replacement therapy (PD, HD, Tx), more severe on PD. 25(OH)D levels have seasonal variations and decreased with time in patients after kidney transplantation.
Validation of a food frequency questionnaire for the assessment of vitamin D intake using the method of triads
Suvi T Itkonen, Maijaliisa Erkkola, Essi Skaffari, Pilvi Saaristo, Elisa M Saarnio, Christel JE Lamberg-Allardt Calcium Research Unit, Division of Nutrition, Department of Food and Environmental Sciences, University of Helsinki, Helsinki, Finland
Osoba prezentująca: Suvi Itkonen ([email protected])
Introduction: The supply of vitamin D-forti- fied dairy products has increased in Finland.
Thus, there is a need to update a tool to assess dietary and supplemental vitamin D intake. The method of triads can be applied to assess the validity of the food frequency questionnaire (FFQ) against food records (FRs) or recalls and biomarker. The method has been less used due to lack of reliable biomarkers on many nutrients.
Purpose of work: We aimed to develop a reliable and valid FFQ with a question on supplementation to assess vitamin D intake in Finland during winter season.
Material and methods: A 98-item FFQ with a separated question about vitamin D supplement use was developed. An interview-administered FFQ, 3-day FR and blood sample for S-25(OH)D analysis were collected from 50 healthy females aged 20-37 years. Validity of the FFQ was assessed as follows: Spearman correlations between the three methods (S-25(OH)D, FR, FFQ) were used to calculate validity coefficients between the hypothetical true intake and the three assessment methods.
Results: FFQ and S-25(OH)D as well FFQ and FR correlated well (r = 0.372, p=0.008 and r = 0.751).
Conclusion: The results are comparable with earlier studies, and the FFQ provides a reasonable estimation of vitamin D intake. The perceived variation in the triads estimates could have been avoided with longer FR period and larger number of subjects.
1. Vitamin D status in children with bronchial asthmaO.V. Tyazhka, Z.V. Selska
Osoba prezentująca: Zoryana Selska ([email protected])
Introduction: It is know nowadays, that vitamin D deficiency may stimulate the progression allergic diseases in human body.
Purpose: Determining the level of 25(OH)D in serum of children with asthma, depending on the severity of the disease.
Materials and methods: We examined 47 children with asthma. In the control group was 60 healthy children. Detecting the 25(OH)D was carried out with the help of ECL methods.
Results: Children with severe persistent asthma severity average 25(OH)D was 16.09 ng/ml (Me = 16.09; Q1 = 12.81; Q3 = 17.57), in children with persistent asthma medium severity - 22.77 ng/ml (Me = 22.77;
Q1 = 17.92; Q3 = 26.79) and in children with a diagnosis of mild persistent asthma severity average 25(OH)D was equal to 32.92 ng/ml (Me = 32.92; Q1 = 29.41; Q3 = 37.31). The children in the control group average of 25(OH)D in serum was 27.79 ng/ml (Me = 27.79; Q1 = 20.94; Q3 = 39.86). A comparison group of children with persistent asthma moderate severity and control group children together was set significantly lower rate of 25(OH)D in the first group.
Conclusions: Thus, there is a correlation between the severity of asthma and the level of 25(OH)D in serum, the heavier the disease occurs the lower the 25(OH)D in serum. Probably Vitamin D is included in the processes of the immune system, aimed at reducing allergic inflammation, because children with asthma need to use vitamin D, particularly challenging children with severe disease.
1. Prevalence of vitamin D deficiency in adult outpatients with schizophrenia or bipolar disorderR. Boerman, D. Cohen, PJ.F Schulte, A. Nugter
Osoba prezentująca: Remco Boerman
Introduction: In adults, insufficient vitamin D levels increase the risk of osteopenia, osteoporosis, and osteomalacia and appear to be associated with psychiatric disorders, such as psychosis, depression, and Alzheimer's disease. Studies in small groups of psychiatric inpatients suggest vitamin D insufficiency to be present, but no properly sized studies have been undertaken. However, we decided to investigate the prevalence of vitamin D insufficiency and deficiency in a large sample of outpatients. Little is known about the prevalence of vitamin D insufficiency in individuals with bipolar disorder. Purpose: To investigate the number of patients with deficiencies.
Methods: All outpatients of three Functional Assertive Community Treatment teams and outpatients of the Centre for Bipolar Disorders were asked to participate in this cross-sectional study.
Results: Vitamin D levels were insufficient in 33% of the patients. 30% of the patients were even deficient (34.9% of those with schizophrenia spectrum disorder and 22.9% of those with bipolar disorder). The type of psychiatric disorder was not a predictor of vitamin D deficiency. The absolute difference in risk of deficiency between the study population and the Dutch Caucasian population was 23.8% (95% CI 18.3-29.3%). Conclusions: There is an increased prevalence of reduced vitamin D levels in outpatients with schizophrenia and bipolar disorder, with a greater, but non-significant, prevalence in schizophrenia. Considering the size of the studied population and the size of the group with the most severe form, 30% of the study population, with vitamin D, we believe that outpatients with schizophrenia, schizoaffective disorder and bipolar disorder can be considered as a new risk group.
1. Rickets in Premature Infants with Very Low Birth Weight: Clinical Features and Course of the DiseaseSvitlana Tkachenko, Yurij Kuzminov, Olha Sheremeta,
Olena Liebiedieva
Osoba prezentująca: Svitlana Tkachenko ([email protected])
Disorders of phosphorus-calcium metabolism and related damage of musculoskeletal apparatus are often observed in premature infants, especially in very and extremely premature ones.
The objective of the research was to determine the features of rickets in very premature infants.
A retrospective clinical examination of 34 premature infants at the age of 1 to 12 months was conducted. The infants were born before 30 weeks' gestation with weight less than 1500 g. Clinical, biochemical, statistical methods were used. Examined children did not get vitamin D3 or got it for a short time.
We have found that 58.8% of children had signs of rickets. It was mainly II degree rickets having acute and sub-acute course. The incidence of rickets depended on gestational age and birth weight. Thus, the incidence of rickets in infants born at 32-33 weeks
(weight 1250-1500 g) constituted 54.5%; in infants delivered at 30-32 weeks (10001249 g) - 67.3%; in infants born before 30 weeks' gestation (less 1000 g) - 97.8%. The features of rickets in premature infants with very low birth weight were an early onset (2nd, 3rd week of life), prevalence of bone changes, mild neurological symptoms; neu- rovegetative symptoms were mild at the onset of the disease, but they intensified at the end of 2-3 months of life. Bone changes manifested in local osteomalacia of temporal regions, napex flattening in sagittal plane, increase in the size of the anterior fontanel. Osteoid tissue enlargement led to formation of the frontal and occipital hills, rachitic "beads” and "bracelets”. Muscular hypotonia was severe.
Thus, rickets in preterm infants has some peculiarities and requires further study of vitamin D3 balance, mechanisms of rachitic process on the background of significant morphofunctional immaturity.
1. The undifferentiated connective tissue dysplasia provide the vitamin D3 for adolescent childrenPochinok T.V., Tyazhka O.V., Zhuravel O.V., Barzylovych V.D.
Osoba prezentująca: Zhuravel O.V. ([email protected])
Introduction: Nowadays, the topic of D-hypovitaminosis and disturbance in metabolism in children still requires further investigation.
Purpose of work: To investigate the level of vitamin D3 in the children with undifferentiated connective tissue dysplasia (UCTD) of juvenile age, by determining the level of 25(OH)D3 venous blood serum.
Patients and Methods: 43 children (21 girls and 22 boys) aged 10 - 16 years: 27 - with NDCTD (13 girls and 15 boys) and 15 children (8 girls and 7 boys) without UCTD determined 25(OH)D3 in the serum of venous blood and hydroxyproline glycosoaminogly- canes in daily urine. A mathematical analysis of the definition of the correlation coefficients was done.
Results: It was found out, that the levels of 25(OH)D3 in the serum of venous blood were significantly reduced in the children with and without UCTD. However, the level of 25(OH)D3 in the children with UCTD was significantly lower (in 81.4% of children with UCTD the level of 25(OH)D3 was below 25 nmol/L) compared with the children without UCTD. Correlation analysis revealed significant inverse relationship between the level of hydroxyproline and 25(OH)D3, which confirms the hypothesis of impaired synthesis of calcium - binding protein and 25-hy- droxycholecalciferol in children with UCTD.
Conclusion: The level of 25(OH)D3 in venous blood serum in the children of juvenile age was significantly reduced. More profound deficiency of vitamin D3 was found in children with UCTD compared with children without UCTD. I n order to prevent the development of various physical processes of children of juvenile age, especially with UCTD it is necessary to prescribe vitamin D3 in the autumn-winter period, in conjunction with a balanced diet.
1. Influence of 1,25(OH)2D3 and its derivatives - PRI-2191 and PRI-2205- on acute-phase protein production in mouse breast cancer Control of the inflammatory process associated with the mammary gland cancer progression by vitamin D and its analoges - PRI-2191, PRI-2205 Agata Pawlik, Joanna Wietrzyk Laboratory of Experimental Anticancer Therapy,
Institute of Immunology and Experimental Therapy, Wrocław Osoba prezentująca: Agata Pawlik ([email protected])
It is known that inflammatory cells can promote cancer development1. The aim of this research is to investigate the hypothesis, that vitamin D can modulate the progression and metastasis of mammary gland cancer via indirect effect on immune response of the host. Therefore, we performed the studies using the 4T1 mouse mammary gland cancer cells, orthotopical- ly transplanted to the immune-competent BALB/c female mice. 4T1 cancer model was chosen, because development of this tumor is followed by great inflammatory response2. On the other hand, these cells, due to low expression of vitamin D receptor (VDR), are invulnerable to active form of vitamin D - calcitriol (1,25(OH)2D3) in vitro. During tumor development mouse were treated with calcitriol (1,25(OH)2D3) and its two analogs - PRI-2191 (natural metabolite of 1,24(OH)2D3, tacalcitol) and PRI-2205 (5, 6-trans isomer of calcipotriol). Both analogs are characterized by significantly reduced toxicity as compared to the calcitriol3. Tumor growth and metastases as well as immune response of the host were monitored at different stages of cancer progression, by collecting samples from established time points of the experiment. Multicolor flow cytometry and cytokine arrays were performed on splenocytes and supernatants from their cultures, respectively. Calcitriol and its
analogs slightly inhibited primary tumor growth, however the metastasis of 4T1 cells to the lungs were increased. Moreover, a tendency to increase the number of regulatory T cells and decrease the level of chemokines from CC family (like CCL11 and CCL17) was observed during treatment.
1. Vitamin d deficiency in patients with subclinical and overt hypothyroidismIvan Pankiv
Bukovinian State Medical Univetsity, Chernivtsi, Ukraine
Osoba prezentująca: Ivan Pankiv ([email protected])
Introduction: There is increasing interest in the role of vitamin D deficiency in a number of chronic health problems including autoimmune diseases. It was reported that patients with Hashimoto's thyroiditis had lower vitamin D levels.
Purpose of work: To investigate the total vitamin 25(OH)D in 70 autoimmune thyroiditis patients with subclinical (n = 21) and overt (n = 49) hypothyroidism.
Material and methods: 70 patients (54 females and 16 males) and 20 apparently healthy individuals with matched age and sex were underwent a detailed clinical examination, thyroid function tests (TSH, fT4, fT3, thyroid peroxidase antibodies) and serum total vitamin 25(OH)D.
Results: The patient group with autoimmune thyroiditis was classified according to the level of TSH into subclinical and overt hypothyroid groups. Levels of serum TSH were significantly increased in subclinical (6.80±1.84 |tIU/ml) and hypothyroid (10.24±2.09 |tIU/ml) groups as compared to control group (2.16±0.39 |tIU/ml). Conclusions: Vitamin 25(OH)D deficiency is associated with autoimmune thyroiditis and further studies are needed to determine whether its deficiency is the causal factor or the consequence of the disease.
1. Vitamin D3 supplementation using an oral spray solution resolves deficiency but has no significant effect on VO2max in Gaelic athletes:** results from a randomised, doubleblind, placebo-controlled trial__Joshua J Todd1, Emeir M McSorley1, L Kirsty Pourshahidi1, Sharon M Madigan2, Eamon Laird3, Martin Healy4,
Pamela J Magee1
Northern Ireland Centre for Food and Health, University of Ulster, Coleraine, Northern Ireland
Irish Institute of Sport, Sports Campus Ireland, Abbotstown, Dublin 15, Ireland
Institute of Molecular Medicine, Trinity College, Dublin, Ireland
Department of Medicine, Trinity Centre for Health Science, St. James's Hospital, Dublin, Ireland
Osoba prezentującą: Joshua J Todd ([email protected])
Abstract: Vitamin D inadequacy is highly prevalent in athletes and whilst the role of vitamin D in skeletal health is well-defined, there remains uncertainty over whether supplementation has an added benefit beyond bone health. This study aimed to determine if vitamin D3 supplementation effects VO2max. Athletes completed a 12-week intervention between November-April 2014/15 and self-administered a single oral spray daily containing 3000IU vitamin D3 (n = 22) or placebo (n = 20). Fasted bloods were analysed for 25-hydroxyvitamin D (25[OH]D)2 and D3 parathyroid hormone, adjusted calcium and creatinine concentrations at baseline and week 12. Athletes also completed VO2max, vertical jump, handgrip strength and lung function tests as well as dietary and physical activity questionnaires. 71% of athletes presented with total 25(OH)D concentrations < 50 nmol/L. Supplementation increased total 25(OH)D concentrations to 81.96 nmol/L, a significant increase compared to athletes on placebo (median change [IQR], 32.69 (46.63) vs 4.64 (11.47) nmol/L respectively; p = 0.006). Compliance to the intervention was 95%. Nevertheless ANCOVA analysis revealed that this had no impact on VO2max (p = 0.375), jump height (p = 0.797), left/right handgrip strength (p = 0.146 and p = 0.266), forced vital capacity (p = 0.573), or forced expiratory volume at 1 second (p = 0.665) when compared to placebo and adjusted for covariates. The high prevalence of vitamin D inadequacy observed in this cohort of collegiate athletes during wintertime supports
the need for vitamin D supplementation to avoid being at risk of poor bone health. Twelve weeks daily supplementation with 3000 IU vitamin D3 successfully resolved deficiency but did not have any significant effect on VO2max, skeletal muscle or lung function in healthy athletes.
1. Maternal obesity and associated vitamin D status in pregnancy: data from the FASSTT studyR. M. Alhomaid, M.S. Mulhern, E. Laird, J.J. Strain,
M.B.E. Livingstone, H. McNulty, K. Pentieva, M.T. McCann
Osoba prezentująca: Raghad Alhomaid ([email protected])
Introduction: Maternal obesity and vitamin D deficiency in pregnancy are both recognised as major public health issues. It has been reported that there is a twofold increase in vitamin D deficiency in pregnant women as maternal BMI increases from 22 to 34 kg/m2.
Aim: To assess maternal vitamin D status (25-hydroxyvitamin D concentrations) among normal weight, overweight, obese.
Methods: Data and samples from a previous study (FASSTT Study) were used for analysis. Pregnant women without pregnancy complications, aged 18 to 35 years and having a singleton pregnancy were included. Participants were not taking any vitamin D containing supplements during pregnancy. Non-fasting blood samples were collected (at 14 and 36 weeks gestation) and were analysed for total serum 25(OH)D using liquid chromatography tandem mass spectrometry.
Results: A total of 216 pregnant women (135 normal weight, 57 overweight, 24 obese) were included in the current analysis. Obese pregnant women had significantly lower median vitamin D status when compared to normal weight women at 14 weeks gestation (32.15 vs.46.10 nmol/L; p = 0.038) but not at 36 weeks (34.65 vs. 42.10 nmol/L; p = 0.370). There was a significant negative correlation between maternal BMI and vitamin D status at 36 weeks gestation (r = -0.201; p = 0.026). At 14 weeks gestation, 60% of participants were either deficient 25(OH)D.
Conclusion: Obese pregnant women are at high risk of vitamin D deficiency. These findings are important for public health agencies when setting recommendations for vitamin D supplementation during pregnancy.
1. immunoglobulin G in children with recurrent respiratory infectionsNel Dąbrowska-Leonik1, Katarzyna Bernat-Sitarz1,
Barbara Pietrucha1, Edyta Heropolitańska-Pliszka1,
Beata Wolska-Kuśnierz1, Małgorzata Pac1, Wiktor Filipiuk2,
Ewa Bernatowska1
Klinika Immunologii, Instytut „Pomnik - Centrum Zdrowia Dziecka', Warszawa
Wydział Elektroniki i Technologii Informatycznych Politechniki Warszawskiej
Osoba prezentująca: Nel Dąbrowska-Leonik ([email protected])
Background: Respiratory infections in children are often connected with attending a nursery school, kindergarten and many siblings. In vitro data show the impact of vitamin D on immune cells. In epidemiological studies vitamin D deficiency is associated with increased incidence of respiratory infection and worse vaccine response. We aimed to assess the correlation between vitamin D, immunoglobulin G (IgG) concentration and level of hepatitis B antibodies in children with recurrent respiratory infections.
Methods: Seven hundred thirty children with recurrent respiratory infections were included to the study. Concentration of serum 25-hydroxyvitamin D (25(OH)D), IgG and an- ti-HBs antibody were measured.
Results: 85% children had the correct levels IgG for age (normal IgG), 11% had IgG above normal (high IgG), only 4% children had low IgG (below reference value for age). 85.9% children had insufficient or deficient 25(OH)D serum concentration. 13.7% had optimal 25(OH)D level. The results were dependent on season and age. Higher 25(OH)D level were on the summer (mean 26.1 ng/ mL) than on the winter (mean 19.26 ng/mL) and higher in younger children 0-2 year of life (mean 27.98 ng/mL) than older, 15-18 years of life (mean 16.17 ng/mL). 25(OH)D level were lower in children with low IgG than with normal IgG: mean 25(OH)D serum concentration 18.04 ng/ml vs 22.51 ng/mL (p = 0.00003). The correlation between 25(OH)D and anti-HBs antibody checked with Pearson test does not indicate existence of any relation (0.1604248).
Conclusions: Optimal level of 25(OH)D presented less than 15% of children with respiratory infection and less than 5% of children with low IgG. Diminished level of IgG is rare cause of recurrent respiratory infections.
1. Vitamin d and cancer diseasesRadka Fuchsova, Ondrej Topolcan, Marie Karlikova,
Vladislav Treska, Andrea Narsanska Osoba prezentująca: Radka Fucchsova ([email protected])
Introduction: Vitamin D is a fat-soluble steroid prohormone which plays a major role in the calcium and phosphorus homeostasis. Vitamin D levels have been associated with many disorders, diseases and related outcomes: osteoporosis, cancer, cardiac risk, autoimmune and rheumatoid diseases, etc. Purpose: To determine the summer and winter levels of vitamin D in patients with different malignant cancer diseases in the Czech Republic. Available data are also presented.
Material and methods: Serum levels of 25- OH vitamin D were measured using CLIA immunoassay developed by Abbott in groups of healthy individuals and in patients with prostate and breast cancer. Serum levels of 230 cancer patients were compared to 250 healthy individuals and the results are evaluated in three groups as deficient, insufficient and sufficient.
Results: Vitamin D levels are more frequently deficient and insufficient in malignant groups than healthy controls.
Conclusion: Authors found a high incidence rate of severe deficiency and insufficiency of vitamin D levels in cancer patients among Czech population. Assessment of vitamin D levels and its supplementation play an important role in the management of patients with different cancer diseases.
This study was supported by the Ministry of Health of the Czech Republic - conceptual development of the University Hospital in Pilsen - FNPl research organization, 00669806 and grants NT-14332-3/2013 and NT-13655-4.
1. Correction of hypovitaminosis D with vitamin D supplements in patients with psoriasisVolha Samakhavets, Ema Ftudenka, Alena Rudenka
Osoba prezentująca: Alena Rudenka ([email protected])
The aim of the study was to determine the prevalence of hypovitaminosis D in patients with psoriatic arthritis (PsA) and cutaneous psoriasis (CP) and evaluate therapeutic effects of vitamin D supplements on dynamics of serum levels of 25(OH)D.
Materials and methods: 88 patients with psoriasis were enrolled in the study: 66 with PsA (34 women and 32 men, mean age 47.1; 10.6 years), 22 (14 women and 8 men, mean age 44.2; 11.9 years) with CP. Control group consisted of 59 healthy volunteers (31 women, 28 men, mean age 46.9; 6.7 years). Clinical examination included assessment of weight, height, severity of skin damage using Psoriasis Area and Severity Index (PASI). Laboratory investigation included evaluation of serum 25(OH)D by electrochemiluminescence technology (Cobas e411) and showings of ESR and CRP. Oil solution of cholecalciferol was used at doses of 2000 IU/day for persons with vitamin D deficiency and 800 IU/day for those with vitamin D insufficiency. Statistical analysis was performed using the software package Statistica 8.0.
1. Association Between Vitamin D and Lipid Accumulation Product in Community Dwelling Elderly PersonsAsta Mastaviciute1, Justina Kilaite2, Marija Tamulaitiene1, Vidmantas Alekna2
Faculty of Medicine, Vilnius University, National Osteoporosis Center, Vilnius, Lithuania
Faculty of Medicine, Vilnius University, Vilnius, Lithuania Osoba prezentująca: Justina Kilaite ([email protected])
Introduction: In recent years papers have suggested the link between vitamin D (25(OH)D) and visceral adiposity. The lipid accumulation product (LAP) is proposed as a marker of dysfunctional adiposity.
Purpose of work: To investigate associations between vitamin D and lipid accumulation product in community dwelling elderly men and women.
Materials and methods: A cross-sectional study was performed on community dwelling elderly persons. Total cholesterol, low density cholesterol, high density cholesterol and triglyceride (TG) concentrations were measured with ADVIA 1800. The level of vitamin D (25(OH)D) was measured with Co- bas E411. Lipid accumulation product (LAP) was calculated as follows: (WC (cm) - 65) x TG (mmol/l)) for men; (WC (cm) - 58 x TG (mmol/l)) for women. Subjects were divided by gender and age every 5 years.
Results: The study was performed on 151 (42.7 %) men and 203 (57.3 %) women. Mean vitamin D was 16.74 ± 10.14 ng/ml and lipid accumulation product - 52.78 ± 36.14 in men group. Mean vitamin D was 16.34 ± 8.14 ng/ ml and mean lipid accumulation product - 48.91 ± 31.0 in women. Moderate statistically significantly positive correlation between vitamin D 25(OH)D and LAP was found in women of 65-69 year (r = 0.406, p = 0.032) and 75-79 year (r = 0.67, p = 0.002). Vitamin D statistically significantly negatively correlated with LAP in 80-84 year women group (r = -0.455, p = 0.013). In all men age groups no statistically significant correlations between vitamin D and LAP were found. Conclusions: There were statistically significant positive correlations between vitamin D and lipid accumulation product in women 65-69 and 75-79 age groups. Vitamin D and LAP statistically significantly negatively correlates in women 80-84 age group.
1. Vitamin D supplementary intake throughout 3rd trimester of pregnancyLazurenko Victoria1, Muryzina Irina1, Hudenko Nataliia2
Department of Obstetrics and Gynaecology N1,
Kharkov National Medical University, Ukraine
Outpatient Gynaecologic Clinic of Kharkov Maternity House N3
Osoba prezentująca: Victoria Lazurenko ([email protected])
Pregnancy is the time when deficiency of any important substance in food intake by mother may result in long-term compromise for foetus future. Vitamin D plays crucial role in Calcium digestion and related to that healthy mineralisation of bones and teeth,
immune protection, state of cardiovascular system, etc. Also it is involved in mechanisms preventing from diabetes mellitus, multiple sclerosis, also it appears to restrain events leading to malignant transformation. It is built in skin in full day measure by exposing to sun for 10 minutes per day. But its production may become insufficient throughout winter especially if 3d trimester happens to take place during this time even in spite of proper food habits. Furthermore food rich of provitamin D is available without restriction not for every Ukrainian women. That is why vitamin D supplement is recommended. The aim of our study was to find out whether the day dose of vitamin D 400 IU is sufficient to provide foetus with proper Calcium supply and its accumulation in tissues but at the same time won't result in kidney impairment. 60 pregnant women were comprised, in a random way 30 (I) of them were prescribed such dose, other 30 (II) just kept recommendation regarding healthy habits. After delivery Calcium was checked in newborn's hair. Kidney function was under tight control. I group appears to show significantly higher content of Calcium in hair without any signs of maternal and neonatal kidney compromise. First year follow-up showed that no child of I group has developed delay in cutting teeth contrariwise to II group (8 cases of delay or other different problems in teething). So we may suggest such approach to implement as widespread and safe for general female population in their 3d trimester of pregnancy.
1. Evaluation of the current vitamin D content of NI milk and its efficacy to increase vitamin D intake of the population through fortificationR.R. Weir1, A.M. Fearon2, J.A.M. Beattie2, S. Stewart2,
M. Johnston3, C. Lowis3, J.J. Strain1, L.K. Pourshahidi1
Northern Ireland Centre for Food and Health (NICHE), University of Ulster, Coleraine, UK
Agri-Food and Biosciences Institute (AFBI), Belfast, UK
Dairy Council for Northern Ireland Shaftesbury House, Edgewater Office Park, Belfast, UK
Osoba prezentująca: Ruth Weir ([email protected])
Introduction: Recent population based surveys indicate that a large proportion of the UK population is vitamin D insufficient, and due to latitude the population is solely
reliant on dietary sources for half the year, however, vitamin D is found in few food sources. One possible strategy to increase vitamin D is through food fortification. In addition the reported concentration of vitamin D within milk maybe out-dated due to changes in husbandry and analysis. Purpose of work: To investigate the current vitamin D content of whole and raw milk produced in NI. Population dietary survey data were manipulated to simulate how vitamin D fortification of milk could improve the dietary intake of vitamin D among the UK population.
Material and methods: Sample of raw and
whole milk were collected for a year and analysed by HPLC for vitamin D content. Results were then added to a dietary model along with three potential fortification levels (1 gg, 1.5 gg and 2 gg per 100 ml) to whole, semi-skimmed, skimmed and one percent milk.
Results: Mean vitamin D3 content for raw milk was 0.08 gg/100 g (SD 0.034) and 0.05 gg/100 g (SD 0.021) for whole milk. The fortification scenario at the highest level (2 gg/100 g) saw a hypothetical increase of vitamin D intake from a median of 2.3 gg/day to 6.1 gg/day for semi-skimmed milk consumers and 1.8 gg/day to 7.4 gg/day for those who reported consuming whole milk.
Conclusions: Results from this study found the vitamin D content in milk to be higher than in some published literature and commonly used food composition tables. It was also found that a milk fortification strategy has the potential to significantly increase the vitamin D intake of the consumer at a population level, which would have a positive knock-on effect on vitamin D status.
1. Can Vitamin D influence BMD in hyperthyroid patients with and without silent vertebral fractures?Ana Paula Barbosa1-4, Mario Rui Mascarenhas1-4, J. Janeiro5,
Isabel Tavora5, Nuno Duarte4, Manuel Bicho2,
Jacinto Monteiro4, Francisco Sampaio4
University Clinic of Endocrinology, Santa Maria Hospital, CHLN-EPE, Lisboa, Portugal
Environmental Health Institute-Faculty of Medicine of Lisbon
CEDML - Clinic of Endocrinology, Diabetes and Metabolism of Lisbon Lda.
Fracturary Osteoporosis Outpatient Clinic- Endocrinology, Diabetes and Metabolism Department
Imagiology Department, Santa Maria Hospital, CHLN-EPE, Lisboa, Portugal
Osoba prezentująca: Ana Paula Barbosa ([email protected])
Hyperthyroidism is associated to BMD reduction, osteoporosis and fragility fractures due to the increase in bone resorption induced by the thyroid hormones. Moreover, changes in vitamin D metabolism can coexist due to nutrients malabsorption and hypercalciuria and can contribute to the increase in the risk of falls.
Objectives: To evaluate the relations between vitamin D, thyroid hormones and BMD in patients with hyperthyroidism, with and without silent vertebral fractures.
Materials and methods: We evaluated 44 patients with hyperthyroidism, 21 men and 23 premenopausal women. Fast blood collection was performed to measure fT3, fT4, TSH, iPTH, calcium, phosphorus and 25(OH)D. BMD (g/cm2) in L1-L4, proximal femur, distal radius and whole body and both lean and fat body masses (Kg) were evaluated by DXA. Vertebral fractures were evaluated by "vertebral fracture assessment” (VFA). No patient was previously treated for hyperthyroidism nor osteoporosis/low bone mass. According the "Institute of Medicine” (IOM), 25(OH)D levels (ng/mL) were divided in deficient (< 20), insufficient (21-29) and normal (> 30). Adequate statistical tests were used. p < 0.05 was considered significant.
Results: The means of the 25(OH)D levels were similar between the groups of patients with (4 men, 5 women) and without fractures, in both sexes. Levels of 25(OH)D in men: deficient - 43%, insufficiency - 33% normal - 24%; women deficient - 35%, insufficiency - 39% normal - 26%.
Significant correlations in men: 25(OH)D and BMD L1-L4 (CC = 0.690; p = 0.0022), femoral neck (CC = 0.503; p = 0.0398) and total femur (CC = 0.554; p = 0.0210); in women 25(OH)D and BMD distal radius (CC = 0,04927; p = 0,0378).
Conclusions: This study suggests that in hyperthyroidism in both sexes there are inadequate levels of vitamin D (around 75%). Moreover, the vitamin D levels seem to influence the cortical bone in both sexes and the trabecular bone in men. These factors can increase bone remodeling and subsequent bone mass loss, which can conjugate in the occurrence of asymptomatic vertebral fractures.