Falls reduced by a third if achieved 40 ng level vitamin D– RCT
Serum 25-hydroxyvitamin D levels and incident falls in older women.
Osteoporos Int. 2018 Sep 25. doi: 10.1007/s00198-018-4705-4. [Epub ahead of print]
Uusi-Rasi K1, Patil R2,3, Karinkanta S2, Tokola K2, Kannus P2,4,5, Lamberg-Allardt C6, Sievänen H2.
1 The UKK Institute for Health Promotion Research, P.O. Box 30, 33501, Tampere, Finland. [email protected].
2 The UKK Institute for Health Promotion Research, P.O. Box 30, 33501, Tampere, Finland.
3 Department of Physiotherapy, Jehangir Hospital, Pune, Maharashtra, 411001, India.
4 Medical School, University of Tampere, Tampere, Finland.
5 Department of Orthopedics and Trauma Surgery, Tampere University Central Hospital, Tampere, Finland.
6 Department of Food and Environmental Sciences, University of Helsinki, Helsinki, Finland.
 1. # Note: It may have taken 6 months to respond. (Many trials last only 3 months)
1. # Note: It may have taken 6 months to respond. (Many trials last only 3 months)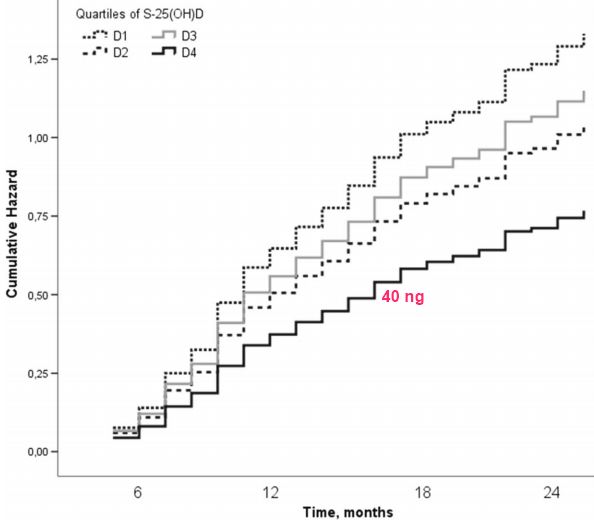 1. # Strangely: Those with D2 response fell less often than D3 1. # Strangely: 26% of women receiving just a placebo had responses of D3 or D4| | | | | || --- | --- | --- | --- | --- || All got 800 IU, but grouped by responses | D1 | D2 | D3 | D4 || Vitamin D response nmol/L | 59.5 | 74.7 | 86.0 | 105.9 (42 ng) || Falls with medically attended injuries | 9.6 | 14.2 | 8.0 | 7.2 || Falls with fractures | 4.1 | 2.7 | 3.4 | 2.0 |Note: They correctly did not record fall data for the first 6 months---* Preventing Falls in Older Adults – Vitamin D combination is the best - JAMA Meta-analysis Nov 2017* Vitamin D prevents falls – majority of meta-analyses conclude – meta-meta analysis Feb 2015* Fallers often had less than 20 ng of vitamin D – meta-analysis April 2014* Added 1 lb of muscle to sarcopenia adults in 13 weeks with just 800 IU vitamin D and protein – RCT Jan 2017* Elderly falls reduced 3.6 times by 900 IU of vitamin D and simple exercise – RCT Nov 2016* Rate of injuries from falls cut in half by just 800 IU of vitamin D and exercise – RCT May 2015
1. # Strangely: Those with D2 response fell less often than D3 1. # Strangely: 26% of women receiving just a placebo had responses of D3 or D4| | | | | || --- | --- | --- | --- | --- || All got 800 IU, but grouped by responses | D1 | D2 | D3 | D4 || Vitamin D response nmol/L | 59.5 | 74.7 | 86.0 | 105.9 (42 ng) || Falls with medically attended injuries | 9.6 | 14.2 | 8.0 | 7.2 || Falls with fractures | 4.1 | 2.7 | 3.4 | 2.0 |Note: They correctly did not record fall data for the first 6 months---* Preventing Falls in Older Adults – Vitamin D combination is the best - JAMA Meta-analysis Nov 2017* Vitamin D prevents falls – majority of meta-analyses conclude – meta-meta analysis Feb 2015* Fallers often had less than 20 ng of vitamin D – meta-analysis April 2014* Added 1 lb of muscle to sarcopenia adults in 13 weeks with just 800 IU vitamin D and protein – RCT Jan 2017* Elderly falls reduced 3.6 times by 900 IU of vitamin D and simple exercise – RCT Nov 2016* Rate of injuries from falls cut in half by just 800 IU of vitamin D and exercise – RCT May 2015PDF is available free at Sci-Hub 10.1007/s00198-018-4705-4
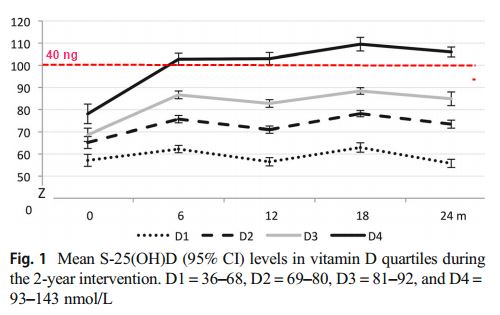
Three hundred eighty-seven home-dwelling older women were divided into quartiles based on mean serum 25-hydroxyvitamin D (S-25(OH)D) levels. The rates of falls and fallers were about 40% lower in the highest S-25(OH)D quartile compared to the lowest despite no differences in physical functioning, suggesting that S-25(OH)D levels may modulate individual fall risk.
INTRODUCTION:
Vitamin D supplementation of 800 IU did not reduce falls in our previous 2-year vitamin D and exercise RCT in 70-80 year old women. Given large individual variation in individual responses, we assessed here effects of S-25(OH)D levels on fall incidence.
METHODS:
Irrespective of original group allocation, data from 387 women were explored in quartiles by mean S-25(OH)D levels over 6-24 months; means (SD) were 59.3 (7.2), 74.5 (3.3), 85.7 (3.5), and 105.3 (10.9) nmol/L. Falls were recorded monthly with diaries. Physical functioning and bone density were assessed annually. Negative binomial regression was used to assess incidence rate ratios (IRRs) for falls and Cox-regression to assess hazard ratios (HR) for fallers. Generalized linear models were used to test between-quartile differences in physical functioning and bone density with the lowest quartile as reference.
RESULTS:
There were 37% fewer falls in the highest quartile, while the two middle quartiles did not differ from reference. The respective IRRs (95% CI) for falls were 0.63 (0.44 to 0.90), 0.78 (0.55 to 1.10), and 0.87 (0.62 to 1.22), indicating lower falls incidence with increasing mean S-25(OH)D levels. There were 42% fewer fallers (HR 0.58; 040 to 0.83) in the highest quartile compared to reference. Physical functioning did not differ between quartiles.
CONCLUSIONS:
Falls and faller rates were about 40% lower in the highest S-25(OH)D quartile despite similar physical functioning in all quartiles. Prevalent S-25(OH)D levels may influence individual fall risk. Individual responses to vitamin D treatment should be considered in falls prevention.