Osteonecrosis of the Jaw might be treated with Vitamin D
Vitamin D Deficiency as a Context-Dependent Modifier of Osteonecrosis of the Jaw - May 2026
Nutrients. 2026 May 30;18(11):1769. doi: 10.3390/nu18111769.
Chien-Lin Lu 1 2, Ren-Yeong Huang 3, Cai-Mei Zheng 4 5 6, Kuo-Cheng Lu 2 7
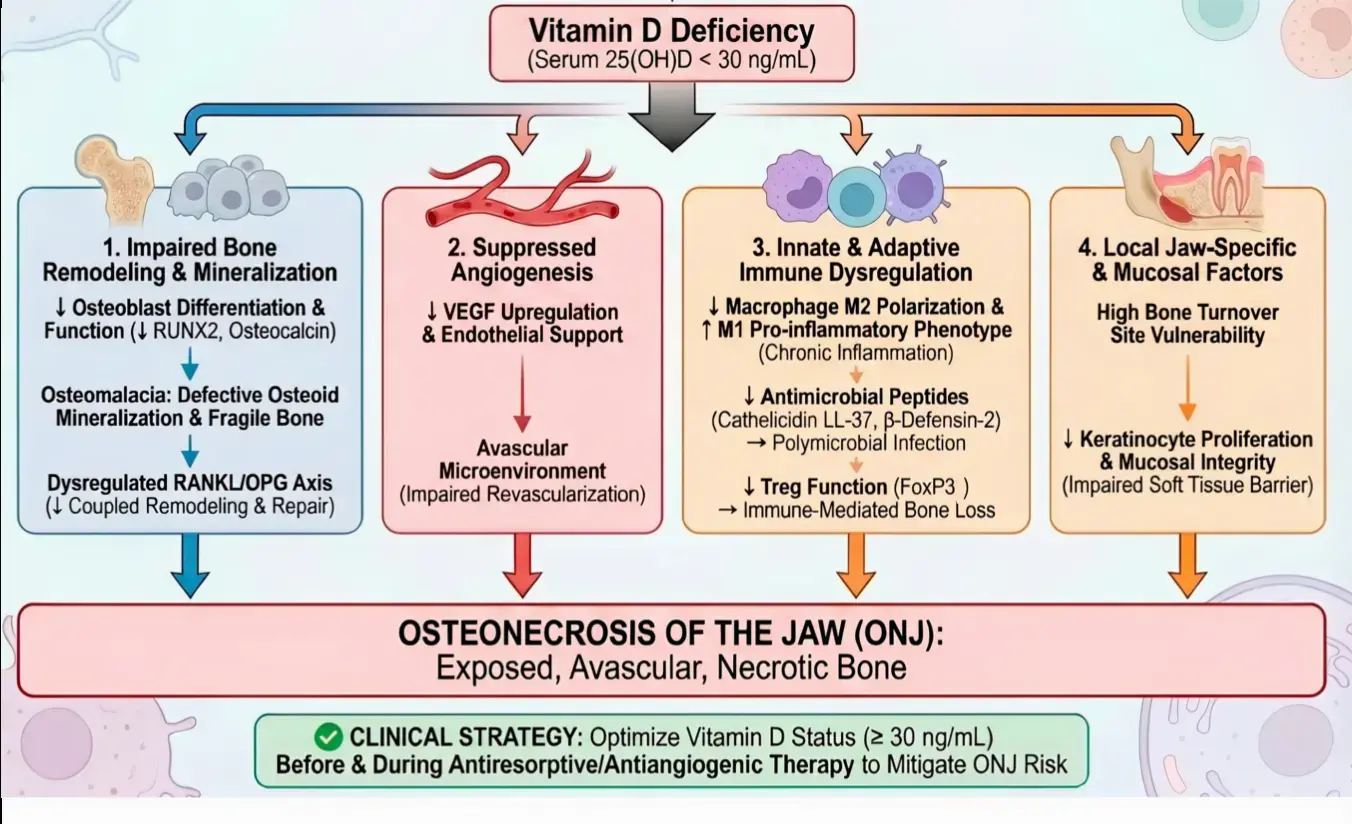
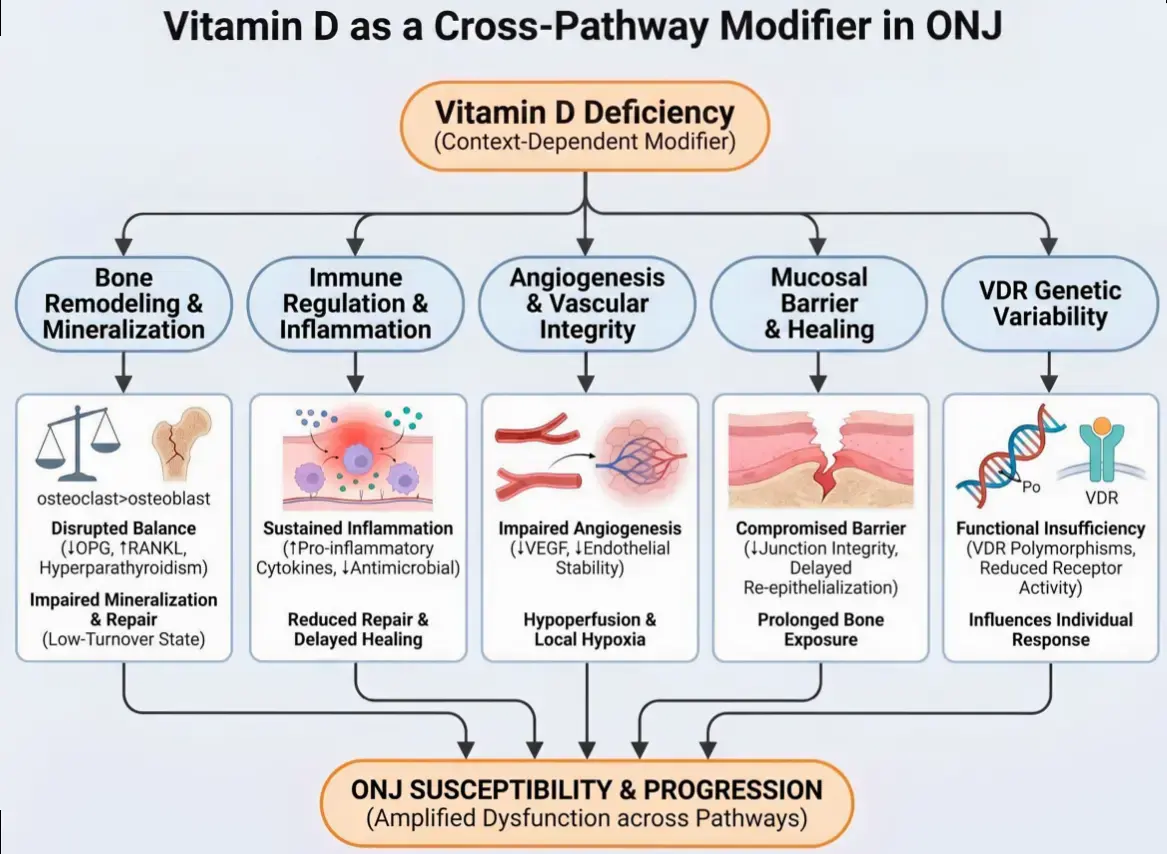
Osteonecrosis of the jaw (ONJ) is a multifactorial disorder characterized by impaired bone remodeling, vascular compromise, immune dysregulation, and mucosal barrier disruption. Although these mechanisms have been extensively investigated, they are often discussed separately, limiting an integrated understanding of ONJ pathogenesis. Vitamin D has emerged as a biologically relevant factor across these interconnected pathways, yet its role in ONJ remains incompletely defined. This narrative and hypothesis-generating review synthesizes current mechanistic, preclinical, observational, and clinical evidence regarding vitamin D biology and ONJ and proposes a vitamin D-centered vulnerability model in which vitamin D deficiency acts as a context-dependent modifier rather than a primary causal driver. Mechanistically, vitamin D deficiency may impair osteoblast function and mineralization, disrupt angiogenic responses, promote pro-inflammatory immune signaling, and compromise mucosal integrity, collectively creating a microenvironment susceptible to impaired healing and osteonecrosis. These effects are likely to vary across clinical settings, particularly in patients receiving antiresorptive or antiangiogenic therapies. Clinical and epidemiological studies have reported associations between low vitamin D status and increased ONJ risk or severity, while some observational studies suggest that vitamin D supplementation may be associated with improved outcomes in selected populations. However, current human evidence remains predominantly observational and subject to substantial heterogeneity and residual confounding, and direct randomized evidence is lacking. Overall, this framework provides an integrated perspective linking vitamin D biology to ONJ-related pathogenic processes and may support future mechanistic research, risk stratification, and supportive multidisciplinary management strategies. Nevertheless, the proposed model should be interpreted cautiously as hypothesis-generating and requires further validation in well-designed prospective studies and randomized controlled trials.
What is ONJ - Claude AI June 2026
Osteonecrosis of the jaw (ONJ) is death of jawbone tissue from compromised blood supply, presenting clinically as exposed, non-healing bone in the mouth.
Why the jaw specifically is the interesting part. Three converging features:
- (1) very high bone turnover in alveolar bone — constant remodeling under masticatory load — which concentrates antiresorptives there;
- (2) the jaw is the only bone separated from a heavily colonized microbial environment by just a thin mucosa, so any breach (a tooth socket) seeds infection directly into bone;
- (3) teeth provide a permanent transcortical conduit. Suppress remodeling and angiogenesis in that setting and healing fails.
ONJ often results from drugs used for Osteoporosis and Cancer
Osteoporosis dosing (low exposure)- Oral bisphosphonates: ~0.01–0.1% (roughly 1 in 1,000 to 1 in 10,000)- IV zoledronate (yearly): similar, low end of the cancer-dose range at most- Denosumab 60 mg q6mo (Prolia): ~0.01–0.03%, comparable to oral BPs- Duration matters even here — risk creeps up past ~4 years of exposure
Cancer dosing (high exposure)- IV zoledronate monthly (bone mets): ~1–2% typical, with reported ranges 0.8–12% depending on duration and how aggressively cases were ascertained- Denosumab 120 mg monthly (Xgeva): ~1–2%, in most head-to-head data marginally higher than zoledronate- Antiresorptive + antiangiogenic combination: higher again- Strong duration dependence — cumulative risk rises sharply after 2–3 years of monthly dosing