Sunlight, Vitamin D and Skin Cancer – 2nd edition
Amazon 2008 edition
Approx $200 for entire book or you can buy individual chapters for about $20
CLICK HERE for the website
The following are abstracts of many of the chapers
Solar Ultraviolet Irradiance and Cancer Incidence and Mortality
William B. Grant
The solar UV‑B (UVB)/vitamin D/cancer hypothesis was proposed by the brothers Cedric and Frank Garland in 1980. In 2002, the list was increased to 15 types of cancer using data in the 1999 version of the atlas of cancer mortality rates in the United States. Ecological studies of cancer incidence and/or mortality rates with respect to indices of solar UVB doses have also been reported for Australia, China, France, Japan, and Spain with largely similar findings. In addition, several studies using nonmelanoma skin cancer as the index of solar UVB dose have found reduced internal cancer incidence and/or mortality rates, especially in sunny countries. A study of cancer incidence with respect to 54 categories of occupation in five Nordic countries, using lip cancer less lung cancer as the UVB index, found this index inversely correlated with 14 types of internal cancers for males and four for females. Observational studies with respect to UVB doses and serum 25‑hydroxyvitamin D [25(OH)D] concentrations also support the hypothesis. Hill’s criteria for causality in a biological system to assess whether solar UVB and vitamin D can be considered causal in reducing risk of cancer. The primary criteria for this analysis include strength of association, consistent findings in different populations, biological gradient, plausibility (e.g., mechanisms), and experimental verification (e.g., randomized controlled trials). The totality of evidence is judged to satisfy the criteria very well for breast and colorectal cancer, and moderately well for several other types of cancer.
UV‑Radiation and Health: Optimal Time for Sun Exposure
Johan Moan, Mantas Grigalavicius, Arne Dahlback, Zivile Baturaite and Asta Juzeniene
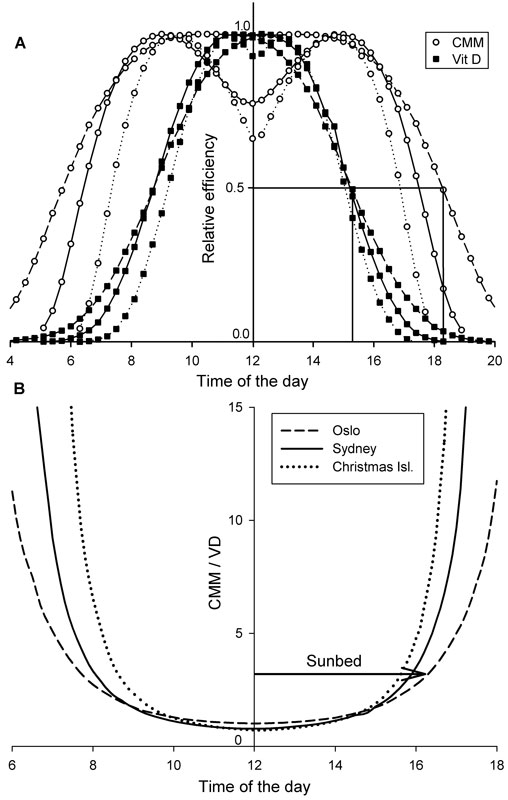
Positive as well as negative health effects of exposure of human skin to UV radiation depend on spectra and fluence rates, both of which being dependent on latitude, time of the day and several other factors. The major positive effects are related to vitamin D photosynthesis and the major negative effect is skin cancer development. The action spectra for these effects are different. This lead us to conclude that for optimal vitamin D synthesis at minimal risk of cutaneous malignant melanoma (CMM), the best time for sun exposure is between 10 a.m. and 1 p.m. Thus, the common health recommendation (that sun exposure should be avoided between the hours of 10 a.m. and 4 p.m. and postponed to the afternoon) may be wrong.
UV Radiation and Cutaneous Malignant Melanoma
Johan E. Moan, Zivile Baturaite, Arne Dahlback and Alina Carmen Porojnicu
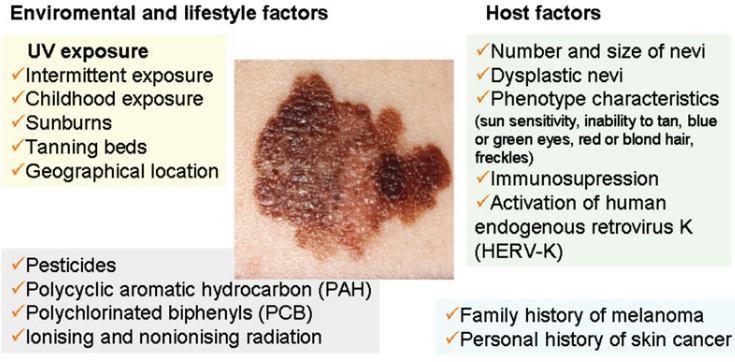
Essential features of the epidemiology and photobiology of cutaneous malignant melanoma (CMM) in Norway were studied in comparison with data from countries at lower latitudes. Arguments for and against a relationship between UV radiation (UV) from sun and artificial light and CMM are discussed. Our data indicate that UV is a carcinogen for CMM and that intermittent exposures are notably melanomagenic. This hypothesis was supported both by latitude gradients, by time trends and by changing patterns of tumor density on different body localizations. However, even though UV radiation generates CMM, it may also have a protective action and/or an action that improves prognosis.
There appears to be no, or even an inverse latitude gradient for CMM arising on non‑UV exposed body localizations (uveal melanoma, CMMs arising in the vulva, perianal/anorectal regions, etc.). Furthermore, CMM prognosis was gradually improved over all years of increasing incidence (up to 1990), but during the past 20 y, incidence rates stabilized and prognosis was not improved significantly.
Comparisons of skin cancer data from Norway, Australia and New Zealand indicate that squamous cell carcinoma and basal cell carcinoma are mainly related to annual solar UVB fluences, while UVA fluences play a larger role of CMM.
Solar UV Exposure and Mortality from Skin Tumors
Marianne Berwick, Claire Pestak and Nancy Thomas
Solar UV radiation (UVR) exposure is clearly associated with increased mortality from non‑melanoma skin cancer—usually squamous cell carcinoma. However, the association with cutaneous melanoma is unclear from the evidence in ecologic studies and several analytic studies have conflicting results regarding the effect of high levels of intermittent UV exposure prior to diagnosis on mortality. Understanding this conundrum is critical to present coherent public health messages and to improve the mortality rates from melanoma.
Sun Exposure and Melanomas on Sun-Shielded and Sun-Exposed Body Areas
Asta Juzeniene, Zivile Baturaite and Johan E. Moan
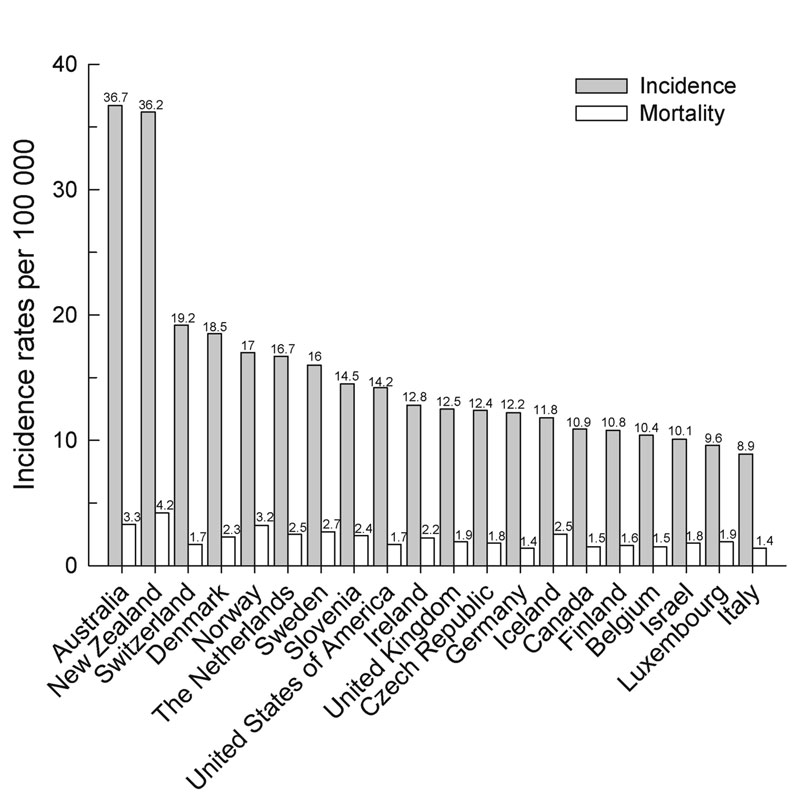
Malignant melanoma is a tumor that arises from melanocytes and accounts for around 4% of all malignancies in Europe and Northern America and for about 11% in Australia and New Zealand. About 10% of primary melanomas arise from sites not exposed to sun. Acral lentiginous melanoma, mucosal melanoma (in the oral cavities, nasal sinuses, genital tract and rectum) and uveal melanoma are all on non‑sun‑exposed tissues. Epidemiologic aspects of melanomas on non‑sun‑exposed areas in comparison with melanomas in sun‑exposed areas have been reviewed. We focus on the relationship between melanoma incidence, geographic latitude of residence, race/ethnicity and host factors as well as time trends.
Vitamin D and Cancer: An Overview on Epidemiological Studies
José Manuel Ordóñez Mena and Hermann Brenner
In recent years, a rapidly increasing number of studies have investigated the relationship of vitamin D with total cancer and site‑specific cancer obtaining diverse findings. In this chapter we provide an overview of epidemiological studies of vitamin D intake, 25‑hydroxyvitamin D and 1,25‑dihydroxyvitamin D serum levels and vitamin D associated polymorphisms in relation to total and site‑specific cancer risk. Overall, epidemiological evidence for total cancer is inconclusive. However, a large number of studies support a relationship of vitamin D with colorectal cancer and to a lesser extent with breast cancer. Findings are inconsistent for other cancers including all other gastrointestinal cancers and prostate cancer. Different vitamin D associated polymorphisms were found to be significantly associated to colorectal, breast and prostate cancer risk.
Protection from UV Damage and Photocarcinogenesis by Vitamin D Compounds
Clare Gordon-Thomson, Wannit Tongkao-on, Eric J Song, Sally E Carter, Katie M Dixon and Rebecca S Mason

Vitamin D is primarily produced by a photochemical reaction in skin, using the energy of ultraviolet B radiation. Ultraviolet radiation in sunlight is also responsible for several types of DNA damage, immunosuppression and photoaging. A number of adaptive responses are known to occur in skin to increasing UV exposure, including increased pigmentation, increased thickness of the cornified layer of skin and upregulation of DNA repair pathways. In addition to these known responses, there is now sufficient evidence to suggest that the local vitamin D system in skin, which includes local production of the active hormone, 1,25dihydroxyvitamin D, together with metabolites of over‑irradiation products, and vitamin D receptor(s), also provide an adaptive response to UV. The vitamin D system in skin reduces DNA damage, inflammation and photocarcinogenesis. Because vitamin D is made in skin, sun damage is less than it would be otherwise.
The Role of Vitamin D for Cardiovascular Disease and Overall Mortality
Armin Zittermann and Sylvana Prokop

In recent years, it became increasingly clear that vitamin D exerts important pleiotropic effects, besides its well‑known effects on extracellular calcium homeostasis and on bone metabolism. This article gives a comprehensive overview of studies on cardiovascular and all‑cause mortality with a focus on the most recent data.
25‑hydroxyvitamin D (25[OH]D) is the best indicator of vitamin D status. Low 25(OH)D levels are highly prevalent among general populations. Prospective cohort studies support the assumption that poor vitamin D status, e.g., 25(OH)D levels below 30 nmol/l, is independently associated with CVD mortality risk. However, support from randomized controlled trials for a beneficial vitamin D effect on CVD risk is still lacking. Meta‑analyses of prospective cohort studies indicate beneficial vitamin D effects on overall mortality as well. There is also likely evidence from meta‑analyses of randomized controlled trials that vitamin D may improve overall mortality in elderly people. Therefore, it is reasonable to supplement institutionalized individuals and other people with deficient 25(OH)D levels with daily vitamin D amounts of 20 µg. However, it is also noteworthy that prospective cohort studies provide evidence for an inverse J‑shaped association between vitamin D status and overall mortality, indicating increased overall mortality risk not only at deficient 25(OH)D levels but also at 25(OH)D levels above 125 nmol/l. Although there is evidence that high 25(OH)D levels sometimes reflect low availability of the vitamin D hormone 1,25‑ dihydroxyvitamin D, future studies are still needed to clarify the association of high 25(OH)D levels with high mortality rates more detailed.
The Vitamin D Receptor: A Tumor Suppressor in Skin
Daniel D. Bikle
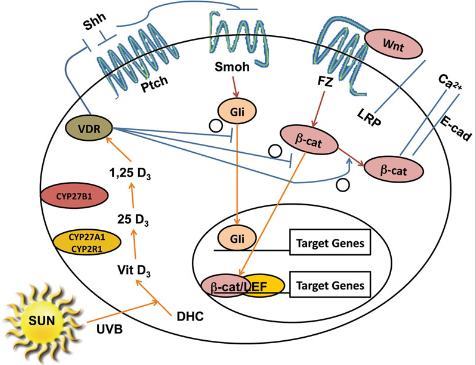
Cutaneous malignancies including melanomas and non melanoma skin cancers (NMSC) are the most common types of cancer, occurring at a rate of over 1 million per year in the United States. The major cell in the epidermis, the keratinocyte, not only produces vitamin D but contains the enzymatic machinery to metabolize vitamin D to its active metabolite, 1,25(OH)2D, and expresses the receptor for this metabolite, the vitamin D receptor (VDR), allowing the cell to respond to the 1,25(OH)2D that it produces. In vitro, 1,25(OH)2D stimulates the differentiation and inhibits the proliferation of these cells and so would be expected to be tumor suppressive. However, epidemiologic evidence demonstrating a negative relationship between circulating levels of the substrate for CYP27B1, 25OHD, and the incidence of these malignancies is mixed, raising the question whether vitamin D is protective in the in vivo setting. UV radiation (UV), both UVB and UVA, as occurs with sunlight exposure is generally regarded as causal for these malignancies, but UVB is also required for vitamin D synthesis in the skin. This complicates conclusions reached from epidemiologic studies in that UVB is associated with higher 25OHD levels as well as increased incidence of cutaneous malignancies. Based on our own data and that reported in the literature we hypothesize that vitamin D signaling in the skin suppresses UVR induced epidermal tumor formation. In this chapter we will first discuss recent data regarding potential mechanisms by which vitamin D signaling suppresses tumor formation, then focus on three general mechanisms that mediate tumor suppression by VDR in the skin: inhibition of proliferation and stimulation of differentiation, immune regulation, and stimulation of DNA damage repair (DDR).
Sunscreens
Guido Bens

Sunscreens have become since more than 40 y the most popular means of protection against UV radiation (UVR) in Western countries. Organic and inorganic filters with different absorption spectrum exist. They filter or scatter UVR. Protection from UVB is quantified as a minimal erythema dose‑based sun protection factor. UVA protection testing is less standardized: Persistent pigment darkening and critical wavelength are currently used methods. Marketing and labeling of sunscreens underlay national regulation which explains major differences between the European and the US sunscreen market. Sunscreens are most performing in sunburn prevention. Broad spectrum UVB and UVA protection and regular application in sufficient amounts are essential for prevention of skin cancers, UV‑induced immunosuppression, and skin aging. A significant benefit from regular sunscreen use has not yet been demonstrated for primary prevention of basal cell carcinoma and melanoma. Concerning the prevention of actinic keratoses, squamous cell carcinomas, and skin aging, the effect of sunscreens is significant, but it remains incomplete. Some organic UV filters (PABA derivatives, cinnamates, benzophenones, and octocrylene) have been described to cause photoallergy. Percutaneous absorption and endocrine disrupting activity of small‑sized organic and nano‑sized inorganic UV filters have been reported. On lesional skin and in pediatric settings, these products should be used with caution. Cutaneous vitamin D synthesis depending on skin‑carcinogenic UVB radiation, the potential risk of vitamin D deficiency by sunscreen use has become a major subject of public health debate. Sunscreens indeed impair vitamin D synthesis if they are used in the recommended amount of 2 mg/cm2, but not in lesser thickness below 1.5 mg/cm2 that corresponds better to what users apply in real life conditions. Large molecular last generation UVB‑UVA broad spectrum sunscreens have a better benefit‑risk ratio than former organic filters: They offer better protection in the UVA band, they are non toxic and non allergenic. A better outcome of sunscreen efficacy especially in primary skin cancer prevention may be achieved with these molecules.
The Role of Vitamin D for Cardiovascular Disease and Overall Mortality
rmin Zittermann and Sylvana Prokop

In recent years, it became increasingly clear that vitamin D exerts important pleiotropic effects, besides its well‑known effects on extracellular calcium homeostasis and on bone metabolism. This article gives a comprehensive overview of studies on cardiovascular and all‑cause mortality with a focus on the most recent data.
25‑hydroxyvitamin D (25[OH]D) is the best indicator of vitamin D status. Low 25(OH)D levels are highly prevalent among general populations. Prospective cohort studies support the assumption that poor vitamin D status, e.g., 25(OH)D levels below 30 nmol/l, is independently associated with CVD mortality risk. However, support from randomized controlled trials for a beneficial vitamin D effect on CVD risk is still lacking. Meta‑analyses of prospective cohort studies indicate beneficial vitamin D effects on overall mortality as well. There is also likely evidence from meta‑analyses of randomized controlled trials that vitamin D may improve overall mortality in elderly people. Therefore, it is reasonable to supplement institutionalized individuals and other people with deficient 25(OH)D levels with daily vitamin D amounts of 20 µg. However, it is also noteworthy that prospective cohort studies provide evidence for an inverse J‑shaped association between vitamin D status and overall mortality, indicating increased overall mortality risk not only at deficient 25(OH)D levels but also at 25(OH)D levels above 125 nmol/l. Although there is evidence that high 25(OH)D levels sometimes reflect low availability of the vitamin D hormone 1,25‑ dihydroxyvitamin D, future studies are still needed to clarify the association of high 25(OH)D levels with high mortality rates more detailed.